

Disease Activity Patterns of Crohn's Disease in the First Ten Years After Diagnosis in the Population-based IBD South Limburg Cohort
- PMID: 32845291
- PMCID: PMC7944516
- DOI: 10.1093/ecco-jcc/jjaa173
Disease Activity Patterns of Crohn's Disease in the First Ten Years After Diagnosis in the Population-based IBD South Limburg Cohort
Abstract
Background and aims: Real-life data on long-term disease activity in Crohn's disease [CD] are scarce. Most studies describe disease course by using proxies, such as drug exposure, need for surgery or hospitalisations, and disease progression. We aimed to describe disease course by long-term disease activity and to identify distinctive disease activity patterns in the population-based IBD South Limburg cohort [IBDSL].
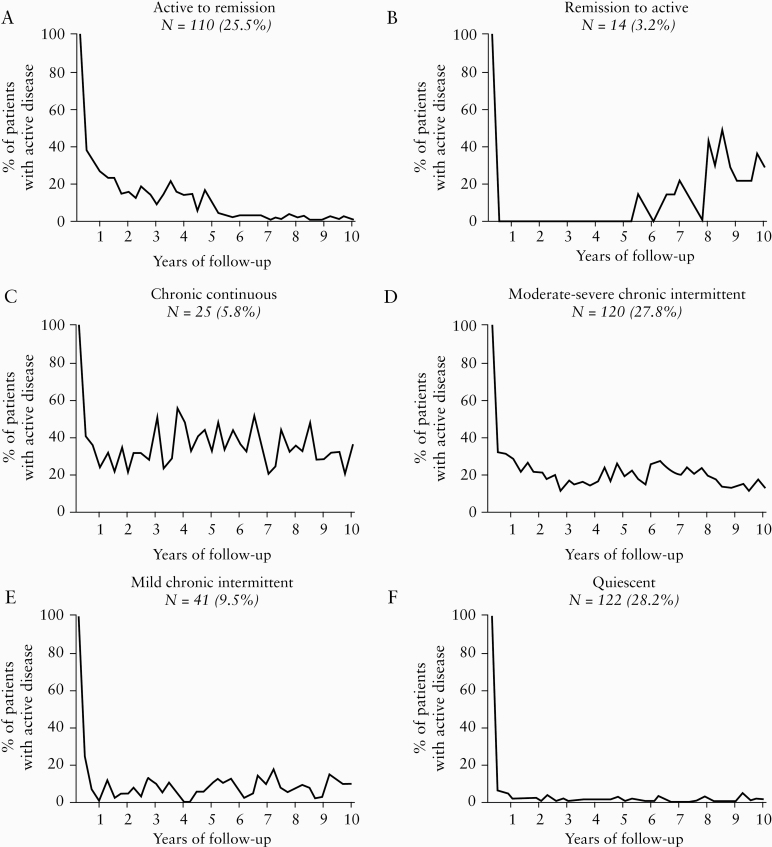
Methods: All CD patients in IBDSL with ≥10 years follow-up [n = 432] were included. Disease activity was defined for each yearly quarter by mucosal inflammation on endoscopy or imaging, hospitalisation, surgery, or treatment adjustment for increased symptoms. Six distinct disease activity clusters were defined. Subsequently, the associations between clinical characteristics and the patterns were assessed using multivariable logistic regression models.
Results: On average, patients experienced 5.44 (standard deviation [SD] 3.96) quarters of disease activity during the first 10 years after diagnosis. Notably, 28.2% of the patients were classified to a quiescent pattern [≤2 active quarters in 10 years], and 89.8% of those never received immunomodulators nor biologics. Surgery at diagnosis (odds ratio [OR] 2.99; 95% confidence interval [CI] 1.07-8.34) and higher age [OR 1.03; 95% CI 1.01-1.06] were positively associated with the quiescent pattern, whereas inverse associations were observed for ileocolonic location [OR 0.44; 95% CI 0.19-1.00], smoking [OR 0.43; 95% CI 0.24-0.76] and need for steroids <6 months [OR 0.24; 95% CI 0.11-0.52].
Conclusions: Considering long-term disease activity, 28.2% of CD patients were classified to a quiescent cluster. Given the complex risk-benefit balance of immunosuppressive drugs, our findings underline the importance of identifying better predictive markers to prevent both over-treatment and under-treatment.
Keywords: Crohn’s disease; Disease course; disease activity; predictive markers; quiescent disease.
© The Author(s) 2020. Published by Oxford University Press on behalf of European Crohn’s and Colitis Organisation.
Figures
References
-
- Jeuring SF, van den Heuvel TR, Liu LY, et al. Improvements in the long-term outcome of Crohn’s disease over the past two decades and the relation to changes in medical management: results from the population-based IBDSL cohort. Am J Gastroenterol 2017;112:325–36. - PubMed
-
- Goldberg R, Irving PM. Toxicity and response to thiopurines in patients with inflammatory bowel disease. Expert Rev Gastroenterol Hepatol 2015;9:891–900. - PubMed
-
- Cohen BL, Sachar DB. Update on anti-tumor necrosis factor agents and other new drugs for inflammatory bowel disease. BMJ 2017;357:j2505. - PubMed
-
- van den Heuvel TR, Wintjens DS, Jeuring SF, et al. Inflammatory bowel disease, cancer and medication: cancer risk in the Dutch population-based IBDSL cohort. Int J Cancer 2016;139:1270–80. - PubMed
-
- Gomollón F, Dignass A, Annese V, et al. ; ECCO . Third European evidence-based consensus on the diagnosis and management of Crohn’s disease 2016. Part 1: diagnosis and medical management. J Crohns Colitis 2017;11:3–25. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
