

A lactate-targeted resuscitation strategy may be associated with higher mortality in patients with septic shock and normal capillary refill time: a post hoc analysis of the ANDROMEDA-SHOCK study
- PMID: 32845407
- PMCID: PMC7450018
- DOI: 10.1186/s13613-020-00732-1
A lactate-targeted resuscitation strategy may be associated with higher mortality in patients with septic shock and normal capillary refill time: a post hoc analysis of the ANDROMEDA-SHOCK study
Abstract
Background: Capillary refill time (CRT) may improve more rapidly than lactate in response to increments in systemic flow. Therefore, it can be assessed more frequently during septic shock (SS) resuscitation. Hyperlactatemia, in contrast, exhibits a slower recovery in SS survivors, probably explained by the delayed resolution of non-hypoperfusion-related sources. Thus, targeting lactate normalization may be associated with impaired outcomes. The ANDROMEDA-SHOCK trial compared CRT- versus lactate-targeted resuscitation in early SS. CRT-targeted resuscitation associated with lower mortality and organ dysfunction; mechanisms were not investigated. CRT was assessed every 30 min and lactate every 2 h during the 8-h intervention period, allowing a first comparison between groups at 2 h (T2). Our primary aim was to determine if SS patients evolving with normal CRT at T2 after randomization (T0) exhibited a higher mortality and organ dysfunction when allocated to the LT arm than when randomized to the CRT arm. Our secondary aim was to determine if those patients with normal CRT at T2 had received more therapeutic interventions when randomized to the LT arm. To address these issues, we performed a post hoc analysis of the ANDROMEDA-SHOCK dataset.
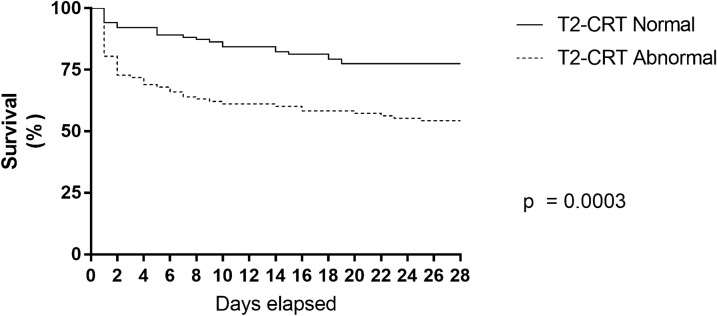
Results: Patients randomized to the lactate arm at T0, evolving with normal CRT at T2 exhibited significantly higher mortality than patients with normal CRT at T2 initially allocated to CRT (40 vs 23%, p = 0.009). These results replicated at T8 and T24. LT arm received significantly more resuscitative interventions (fluid boluses: 1000[500-2000] vs. 500[0-1500], p = 0.004; norepinephrine test in previously hypertensive patients: 43 (35) vs. 19 (19), p = 0.001; and inodilators: 16 (13) vs. 3 (3), p = 0.003). A multivariate logistic regression of patients with normal CRT at T2, including APACHE-II, baseline lactate, cumulative fluids administered since emergency admission, source of infection, and randomization group) confirmed that allocation to LT group was a statistically significant determinant of 28-day mortality (OR 3.3; 95%CI[1.5-7.1]); p = 0.003).
Conclusions: Septic shock patients with normal CRT at baseline received more therapeutic interventions and presented more organ dysfunction when allocated to the lactate group. This could associate with worse outcomes.
Keywords: Capillary refill time; Early resuscitation; Lactate; Peripheral perfusion; Sepsis; Septic shock.
Conflict of interest statement
All authors declare no conflict of interest.
Figures


References
-
- Hernandez G, Ospina-Tascon G, Petri Damiani L, Estenssoro E, Dubin A, Hurtado J, et al. Effect of a resuscitation strategy targeting peripheral perfusion status vs serum lactate levels on 28-day mortality among patients with septic shock The ANDROMEDA-SHOCK Randomized Clinical Trial. JAMA. 2019;321:654–664. doi: 10.1001/jama.2019.0071. - DOI - PMC - PubMed
-
- Zampieri FG, Damiani LP, Bakker J, Ospina-Tascón GA, Castro R, Cavalcanti AB, et al. Effect of a resuscitation strategy targeting peripheral perfusion status vs serum lactate levels on 28-day mortality among patients with septic shock: a bayesian reanalysis of the ANDROMEDA-SHOCK Trial. Am J Respir Crit Care Med. 2019 doi: 10.1164/rccm.201905-0968OC. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
