

Perspectives on Triple-Negative Breast Cancer: Current Treatment Strategies, Unmet Needs, and Potential Targets for Future Therapies
- PMID: 32846967
- PMCID: PMC7565566
- DOI: 10.3390/cancers12092392
Perspectives on Triple-Negative Breast Cancer: Current Treatment Strategies, Unmet Needs, and Potential Targets for Future Therapies
Abstract
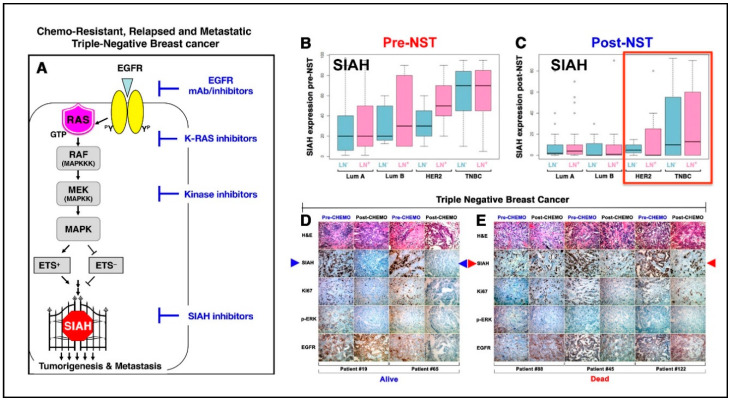
Triple-negative breast cancer (TNBC), characterized by the absence or low expression of estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor (HER2), is the most aggressive subtype of breast cancer. TNBC accounts for about 15% of breast cancer cases in the U.S., and is known for high relapse rates and poor overall survival (OS). Chemo-resistant TNBC is a genetically diverse, highly heterogeneous, and rapidly evolving disease that challenges our ability to individualize treatment for incomplete responders and relapsed patients. Currently, the frontline standard chemotherapy, composed of anthracyclines, alkylating agents, and taxanes, is commonly used to treat high-risk and locally advanced TNBC. Several FDA-approved drugs that target programmed cell death protein-1 (Keytruda) and programmed death ligand-1 (Tecentriq), poly ADP-ribose polymerase (PARP), and/or antibody drug conjugates (Trodelvy) have shown promise in improving clinical outcomes for a subset of TNBC. These inhibitors that target key genetic mutations and specific molecular signaling pathways that drive malignant tumor growth have been used as single agents and/or in combination with standard chemotherapy regimens. Here, we review the current TNBC treatment options, unmet clinical needs, and actionable drug targets, including epidermal growth factor (EGFR), vascular endothelial growth factor (VEGF), androgen receptor (AR), estrogen receptor beta (ERβ), phosphoinositide-3 kinase (PI3K), mammalian target of rapamycin (mTOR), and protein kinase B (PKB or AKT) activation in TNBC. Supported by strong evidence in developmental, evolutionary, and cancer biology, we propose that the K-RAS/SIAH pathway activation is a major tumor driver, and SIAH is a new drug target, a therapy-responsive prognostic biomarker, and a major tumor vulnerability in TNBC. Since persistent K-RAS/SIAH/EGFR pathway activation endows TNBC tumor cells with chemo-resistance, aggressive dissemination, and early relapse, we hope to design an anti-SIAH-centered anti-K-RAS/EGFR targeted therapy as a novel therapeutic strategy to control and eradicate incurable TNBC in the future.
Keywords: Cytoxan; EGFR/K-RAS/SIAH signaling pathway; and Taxotere); chemo-resistance; clinical diagnostics; concurrent ACT regimen (Adriamycin; improved patient survival; neoadjuvant chemotherapy (NACT); pathologic incomplete responders (pIR); prognostics; residual cancer burden (RCB); sequential ACT regimen (AC-T); triple-negative breast cancer (TNBC); tumor recurrence; tumor-driving signaling pathways in TNBC.
Conflict of interest statement
The authors describe no conflict of interests.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
