

Early experience utilizing artificial intelligence shows significant reduction in transfer times and length of stay in a hub and spoke model
- PMID: 32847449
- PMCID: PMC7645178
- DOI: 10.1177/1591019920953055
Early experience utilizing artificial intelligence shows significant reduction in transfer times and length of stay in a hub and spoke model
Abstract
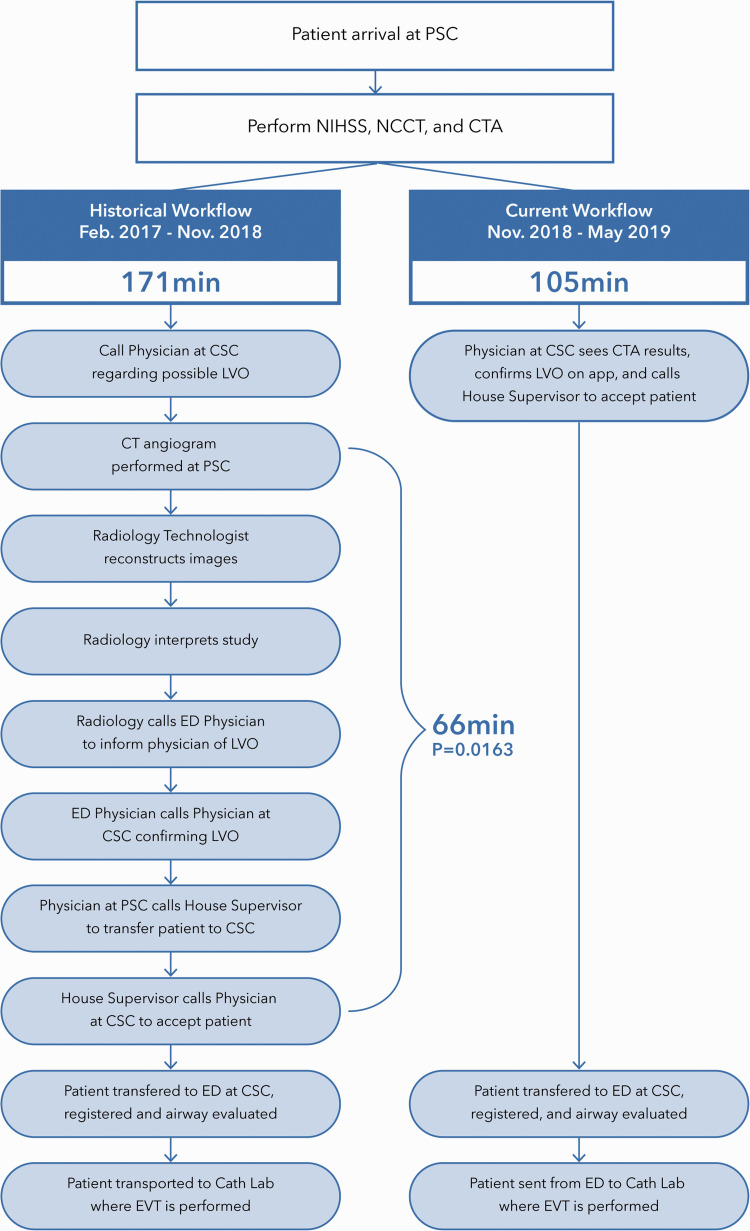
Background: Recently approved artificial intelligence (AI) software utilizes AI powered large vessel occlusion (LVO) detection technology which automatically identifies suspected LVO through CT angiogram (CTA) imaging and alerts on-call stroke teams. We performed this analysis to determine if utilization of AI software and workflow platform can reduce the transfer time (time interval between CTA at a primary stroke center (PSC) to door-in at a comprehensive stroke center (CSC)).
Methods: We compared the transfer time for all LVO transfer patients from a single spoke PSC to our CSC prior to and after incorporating AI Software (Viz.ai LVO). Using a prospectively collected stroke database at a CSC, demographics, mRS at discharge, mortality rate at discharge, length of stay (LOS) in hospital and neurological-ICU were examined.
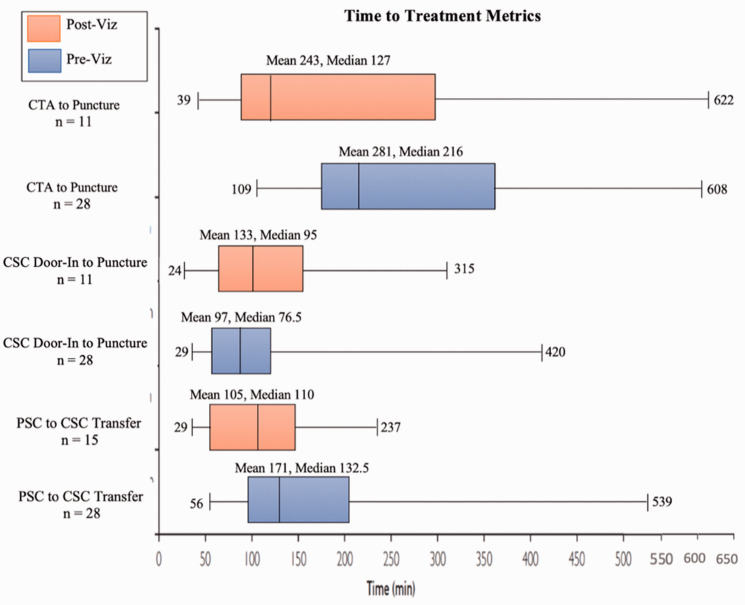
Results: There were a total of 43 patients during the study period (median age 72.0 ± 12.54 yrs., 51.16% women). Analysis of 28 patients from the pre-AI software (median age 73.5 ± 12.28 yrs., 46.4% women), and 15 patients from the post-AI software (median age 70.0 ± 13.29 yrs., 60.00% women). Following implementation of AI software, median CTA time at PSC to door-in at CSC was significantly reduced by an average of 22.5 min. (132.5 min versus 110 min; p = 0.0470).
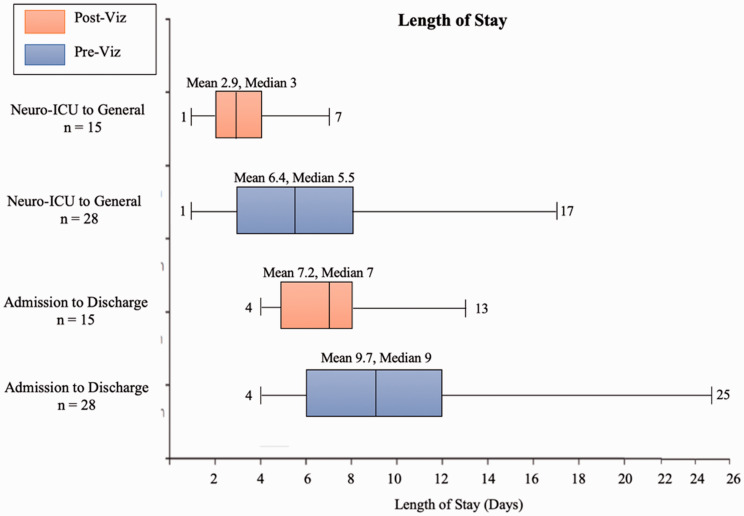
Conclusions: The incorporation of AI software was associated with an improvement in transfer times for LVO patients as well as a reduction in the overall hospital LOS and LOS in the neurological-ICU. More extensive studies are warranted to expand on the ability of AI technology to improve transfer times and outcomes for LVO patients.
Keywords: CT angiography; Intervention; artificial intelligence; stroke.
Conflict of interest statement
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: AEH: Consultant for Medtronic, Microvention, Penumbra, Stryker, Genentech, Balt, Viz.ai, and GE Healthcare.
Figures
References
-
- Kunz WG, Almekhlafi MA, Menon BK, et al. Public health and cost consequences of treatment delays in endovascular thrombectomy for stroke based on HERMES collaboration data. Eur Stroke J 2018; 15: 587–620.
-
- Froehler MT, Jeffrey LS, Zaidat OO, et al. Interhospital transfer before thrombectomy is associated with delayed treatment and worse outcome in the STRATIS registry (systematic evaluation of patients treated with neurothrombectomy devices for acute ischemic stroke). AHA J 2017; 136: 2311–2321. - PMC - PubMed
-
- Goyal M, Jadhav AP, Bonafe A, for the SWIFT PRIME investigators et al. Analysis of workflow and time to treatment and the effects on outcome in endovascular treatment of acute ischemic stroke: results from the SWIFT PRIME randomized controlled trial. Radiology 2016; 279: 888–897. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
