

Myofibroma/myofibromatosis: MDCT and MR imaging findings in 24 patients with radiological-pathological correlation
- PMID: 32847537
- PMCID: PMC7449012
- DOI: 10.1186/s12880-020-00498-9
Myofibroma/myofibromatosis: MDCT and MR imaging findings in 24 patients with radiological-pathological correlation
Abstract
Background: The aim of this study was to characterize the radiological features of myofibroma on multidetector computed tomography (MDCT) and magnetic resonance imaging (MRI) and correlate the imaging findings with pathologic features.
Methods: The radiological findings of 24 patients with 29 myofibromas were retrospectively reviewed. All images were evaluated with emphasis on density, signal intensity, hypointense area, and enhancement, correlating these with pathologic findings.
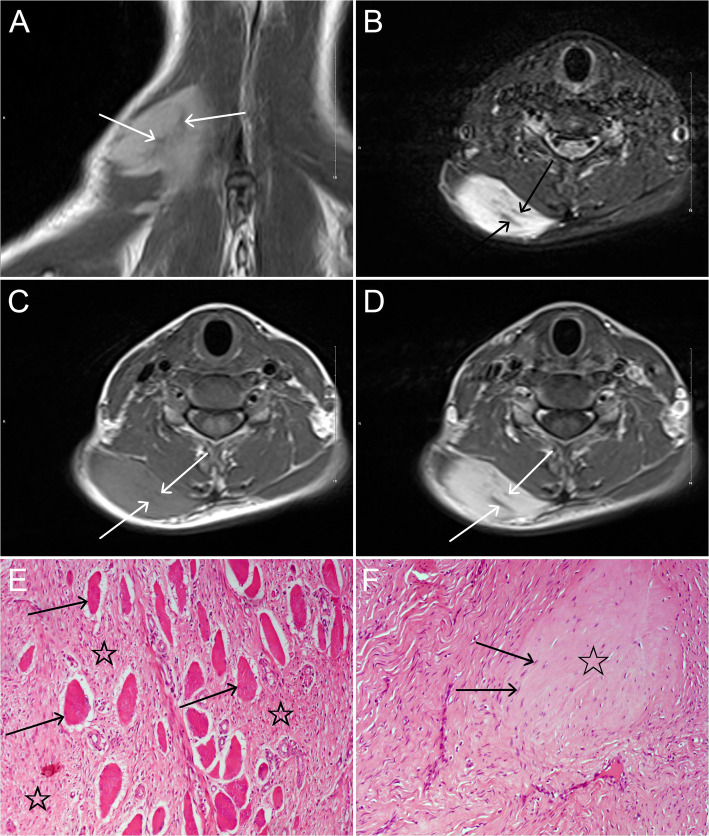
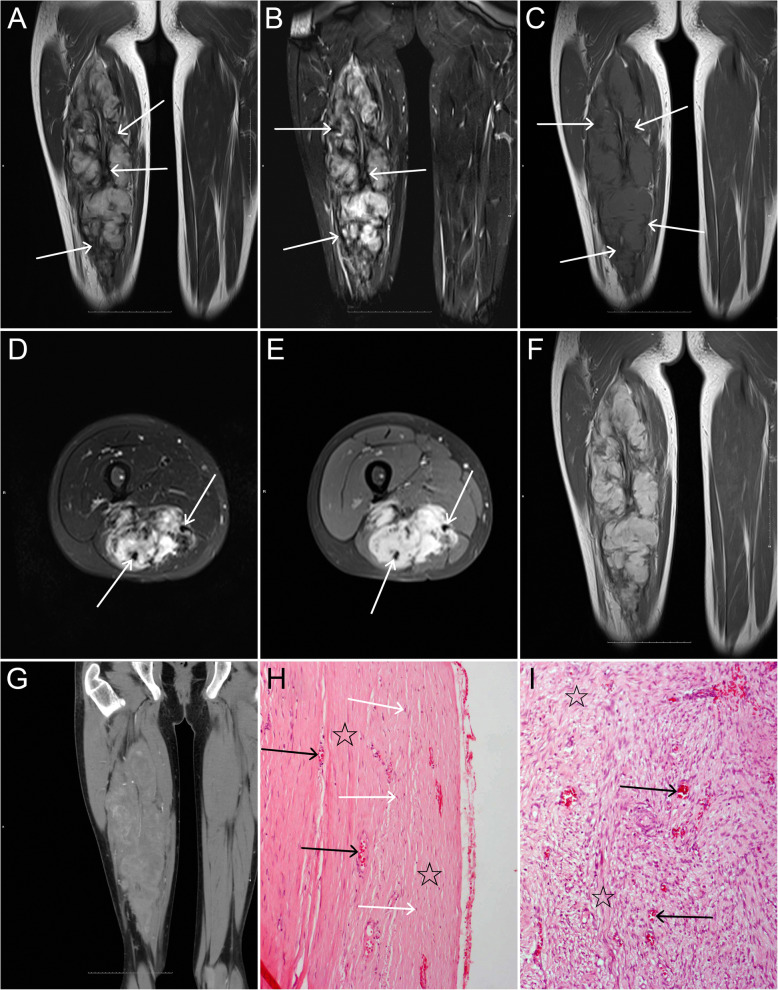
Results: On plain MDCT scan, 4(26.7%) tumors were homogeneous isodensity, 4(26.7%) tumors were heterogeneous hyperdensity, and 7(46.7%) tumors were heterogeneous hypodensity. On contrast-enhanced MDCT scan, all tumors (9/9) showed heterogeneous enhancement with moderate in 3(33.3%) and marked in 6(66.7%) tumors, and their enhancements were higher compared to adjacent skeletal muscle (P = 0.0001). On MRI, heterogeneous slight hyperintensity, homogeneous slight hyperintensity, and heterogeneous hypointensity on T1-weighted imaging (T1WI) were observed in 14(82.3%), 1(5.9%) and 2(11.8%) tumors, respectively. On T2-weighted imaging (T2WI) and fat-suppressed (FS) T2WI, all tumors demonstrated heterogeneous hyperintensity. All tumors showed heterogeneous marked enhancement on FS contrast-enhanced T1WI. On T1WI, T2WI, FS T2WI, and FS contrast-enhanced T1WI, irregular strip or/and patchy hypointensities were found in 16(94.1%), 12(100%), 17(100%) and 17(100%) tumors, respectively, and pseudocapsule was seen in 5(29.4%) tumors. The hypointensities and pseudocapsule on MRI were exactly corresponding to pathological interlacing collagen fibers and fibrosis. The age of the recurrent group was lower than that of the non-recurrent group (P = 0.001) and the tumors without pseudocapsule were more likely to recur than those with pseudocapsule (P = 0.034).
Conclusion: Myofibromas are characterized by heterogeneous density or signal intensity, with moderate or marked enhancement. The hypointensities and pseudocapsule on MRI may be helpful in diagnosis, and the absence of pseudocapsule and younger age may be risk factors for tumor recurrence.
Keywords: Magnetic resonance imaging; Multidetector computed tomography; Myofibroma; Myofibromatosis; Pathology.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Fletcher CD, Hogendoorn PC, Mertens F, Bridge J. WHO classification of tumors of soft tissue and bone. 4. Lyon: IARC Press; 2013.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
