

The impact of order with radiation therapy in stage IIIA pathologic N2 NSCLC patients: a population-based study
- PMID: 32847544
- PMCID: PMC7448510
- DOI: 10.1186/s12885-020-07309-y
The impact of order with radiation therapy in stage IIIA pathologic N2 NSCLC patients: a population-based study
Abstract
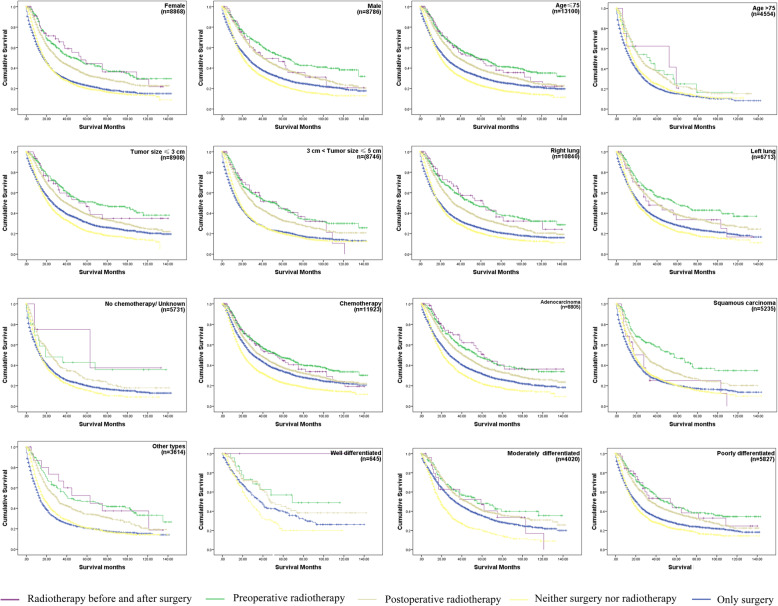
Background: The aim of this study was to investigate the optimal order of radiation therapy in patients affected by stage IIIA pathologic N2 (IIIA/N2) non-small-cell lung cancer (NSCLC) and to identify its potential risk factors.
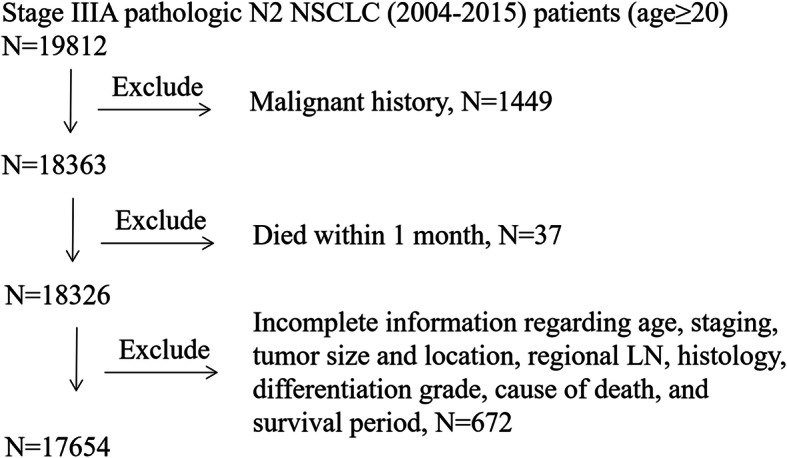
Methods: 17,654 (8786 men and 8868 women) diagnosed with NSCLC stage IIIA-N2 from 2004 to 2015 patients were identified in the Surveillance, Epidemiology, and End Results (SEER) database. Among the relevant clinical parameters, we evaluated overall survival (OS), lung cancer-specific survival (LCSS) and other variables such as age, sex and tumor size in patients who were treated with different combinations of surgery and radiotherapy strategies.
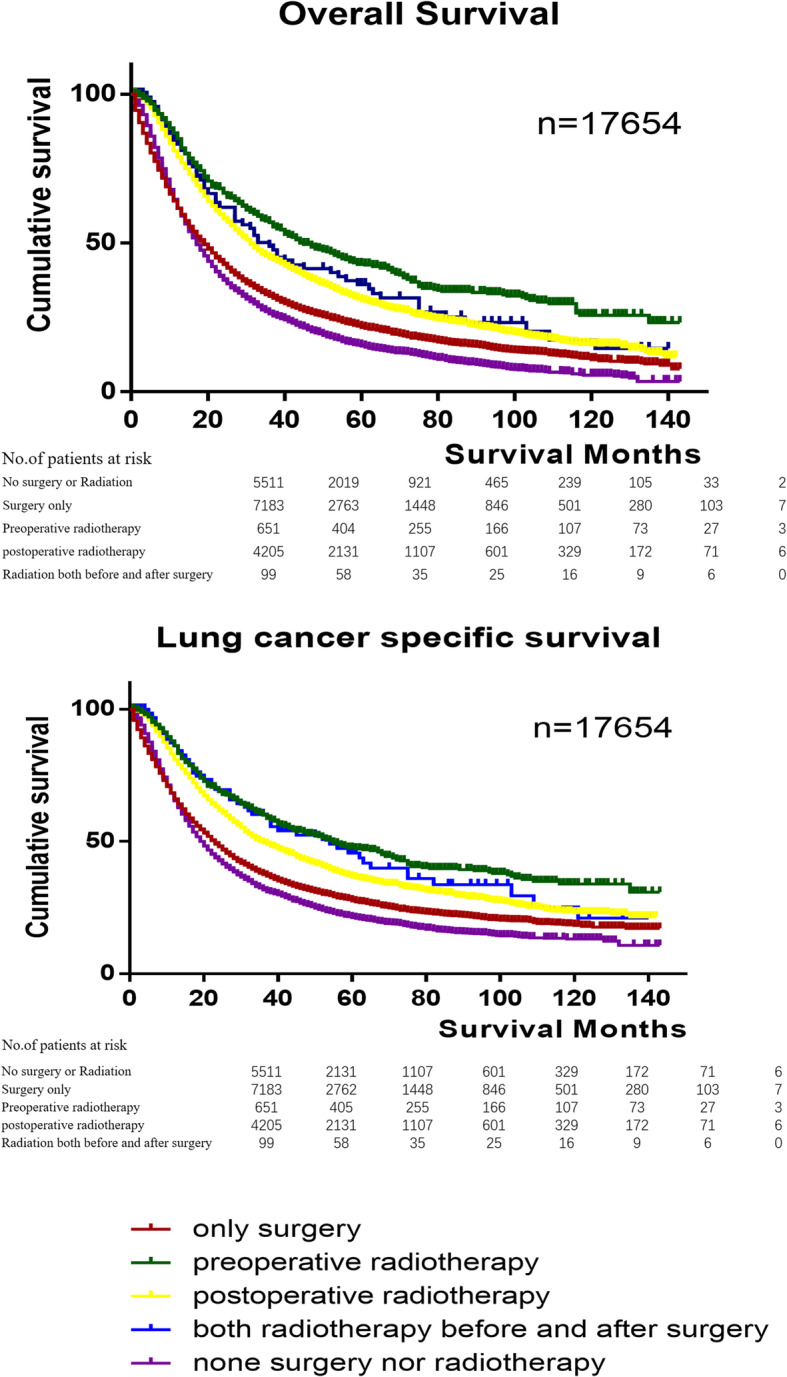
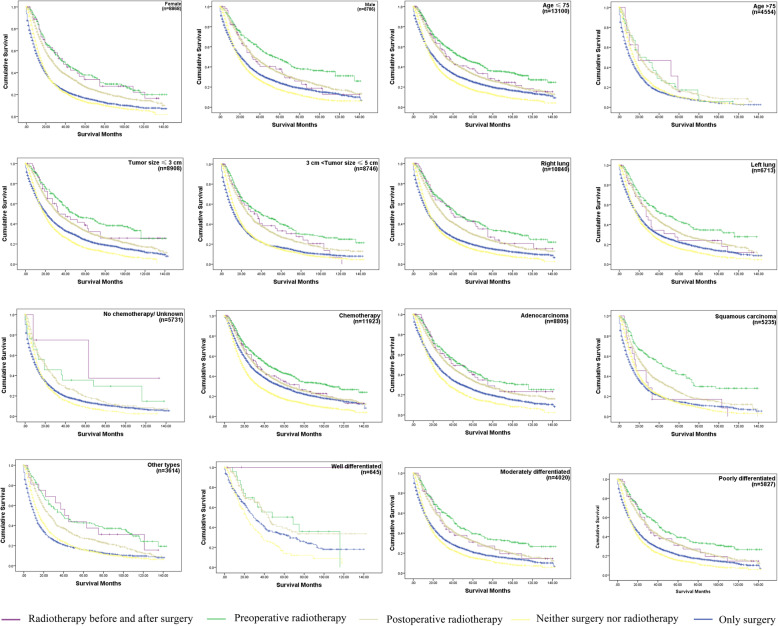
Results: We discovered that surgery benefit in younger IIIA/N2 NSCLC patients (age ≤ 75), and compared with surgery only, preoperative radiotherapy significantly improved the survival rate most (p < 0.001). When we performed the OS and LCSS analysis in the subgroup of patients' age > 75 years old, who underwent postoperative radiotherapy (PORT) had the highest survival rate (p < 0.001). Multivariate analyses showed that the following parameters had a negative impact on survival: female sex, older age, no chemotherapy, large tumor size, high tumor grade, no surgery or radiotherapy.
Conclusions: In IIIA/N2 NSCLC patients, surgery, radiotherapy and chemotherapy were associated with improved OS and LCSS. Younger patients underwent surgical resection and chemotherapy, the main population we studied, benefited most from preoperative radiotherapy in all orders with radiation therapy (p < 0.001). In patients more than 75 years old, there was no clear benefit from only surgery, and PORT was recommended in case of having surgery.
Keywords: Non-small-cell lung carcinoma; Radiotherapy; SEER; Surgery; Survival.
Conflict of interest statement
The authors declare no potential conflicts of interest related to this study.
Figures
References
-
- Sawabata N, Miyaoka E, Asamura H, Nakanishi Y, Eguchi K, Mori M, Nomori H, Fujii Y, Okumura M, Yokoi K, R. Japanese Joint Committee for Lung Cancer Japanese lung cancer registry study of 11,663 surgical cases in 2004: demographic and prognosis changes over decade. J Thorac Oncol. 2011;6(7):1229–1235. doi: 10.1097/JTO.0b013e318219aae2. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
