

Management of Latent Autoimmune Diabetes in Adults: A Consensus Statement From an International Expert Panel
- PMID: 32847960
- PMCID: PMC7809717
- DOI: 10.2337/dbi20-0017
Management of Latent Autoimmune Diabetes in Adults: A Consensus Statement From an International Expert Panel
Abstract
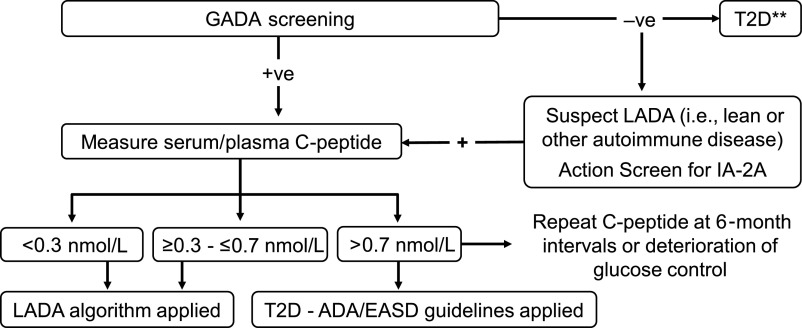
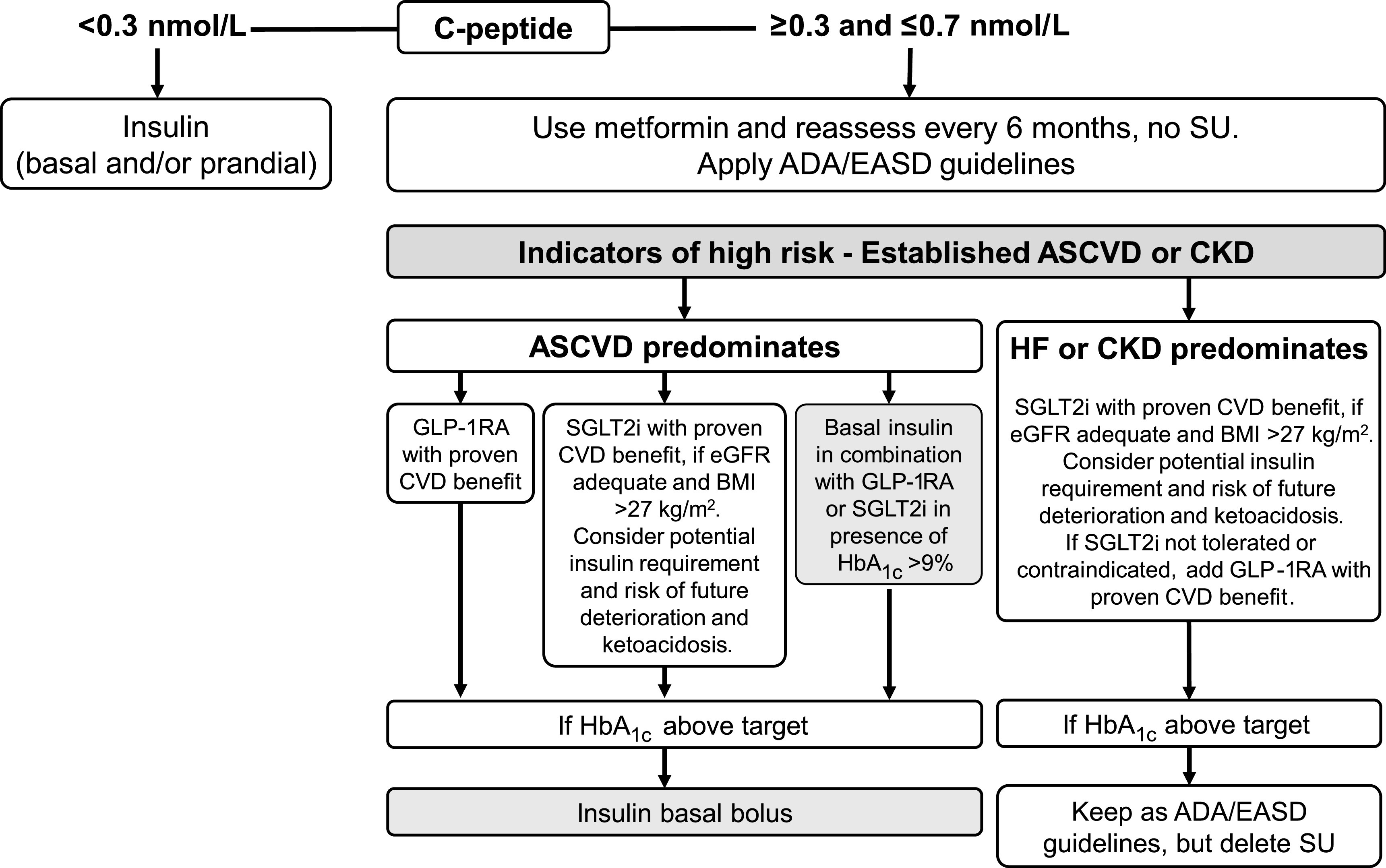
A substantial proportion of patients with adult-onset diabetes share features of both type 1 diabetes (T1D) and type 2 diabetes (T2D). These individuals, at diagnosis, clinically resemble T2D patients by not requiring insulin treatment, yet they have immunogenetic markers associated with T1D. Such a slowly evolving form of autoimmune diabetes, described as latent autoimmune diabetes of adults (LADA), accounts for 2-12% of all patients with adult-onset diabetes, though they show considerable variability according to their demographics and mode of ascertainment. While therapeutic strategies aim for metabolic control and preservation of residual insulin secretory capacity, endotype heterogeneity within LADA implies a personalized approach to treatment. Faced with a paucity of large-scale clinical trials in LADA, an expert panel reviewed data and delineated one therapeutic approach. Building on the 2020 American Diabetes Association (ADA)/European Association for the Study of Diabetes (EASD) consensus for T2D and heterogeneity within autoimmune diabetes, we propose "deviations" for LADA from those guidelines. Within LADA, C-peptide values, proxy for β-cell function, drive therapeutic decisions. Three broad categories of random C-peptide levels were introduced by the panel: 1) C-peptide levels <0.3 nmol/L: a multiple-insulin regimen recommended as for T1D; 2) C-peptide values ≥0.3 and ≤0.7 nmol/L: defined by the panel as a "gray area" in which a modified ADA/EASD algorithm for T2D is recommended; consider insulin in combination with other therapies to modulate β-cell failure and limit diabetic complications; 3) C-peptide values >0.7 nmol/L: suggests a modified ADA/EASD algorithm as for T2D but allowing for the potentially progressive nature of LADA by monitoring C-peptide to adjust treatment. The panel concluded by advising general screening for LADA in newly diagnosed non-insulin-requiring diabetes and, importantly, that large randomized clinical trials are warranted.
© 2020 by the American Diabetes Association.
Figures

References
-
- Di Mario U, Irvine WJ, Borsey DQ, Kyner JL, Weston J, Galfo C. Immune abnormalities in diabetic patients not requiring insulin at diagnosis. Diabetologia 1983;25:392–395 - PubMed
-
- Groop LC, Bottazzo GF, Doniach D. Islet cell antibodies identify latent type I diabetes in patients aged 35-75 years at diagnosis. Diabetes 1986;35:237–241 - PubMed
-
- Tuomi T, Groop LC, Zimmet PZ, Rowley MJ, Knowles W, Mackay IR. Antibodies to glutamic acid decarboxylase reveal latent autoimmune diabetes mellitus in adults with a non-insulin-dependent onset of disease. Diabetes 1993;42:359–362 - PubMed
-
- Turner R, Stratton I, Horton V, et al. .; UK Prospective Diabetes Study Group . UKPDS 25: autoantibodies to islet-cell cytoplasm and glutamic acid decarboxylase for prediction of insulin requirement in type 2 diabetes. Lancet 1997;350:1288–1293 - PubMed
-
- Tuomi T, Carlsson A, Li H, et al. . Clinical and genetic characteristics of type 2 diabetes with and without GAD antibodies. Diabetes 1999;48:150–157 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
