

Biomechanical Changes to the Cornea from LASIK Flap Creation Resulting in Inaccurate Ablations and Suboptimal Refractive Outcomes with Topographic-Guided Ablation
- PMID: 32848360
- PMCID: PMC7429235
- DOI: 10.2147/OPTH.S263896
Biomechanical Changes to the Cornea from LASIK Flap Creation Resulting in Inaccurate Ablations and Suboptimal Refractive Outcomes with Topographic-Guided Ablation
Abstract
Purpose: This study documents a biomechanical corneal change related to corneal flap creation in certain patients leading to an irregular ablation pattern and an inaccurate refractive outcome.
Methods: This retrospective study included consecutive eyes treated with primary LASIK Contoura using the LYRA Protocol. All LASIK procedures were performed on the WaveLight EX500 excimer laser. Flaps were created with either the Alcon WaveLight FS200 femtosecond laser or the Moria M2 microkeratome. Eyes that were off by greater than or equal to 0.50 diopters (D) sphere or cylinder from the targeted goal within 3 months after surgery were identified. Topographical, higher order aberration, and epithelial maps were created. Of these eyes, approximately 10% of eyes were found to have undergone a biomechanical change upon flap creation that led to an inaccurate outcome.
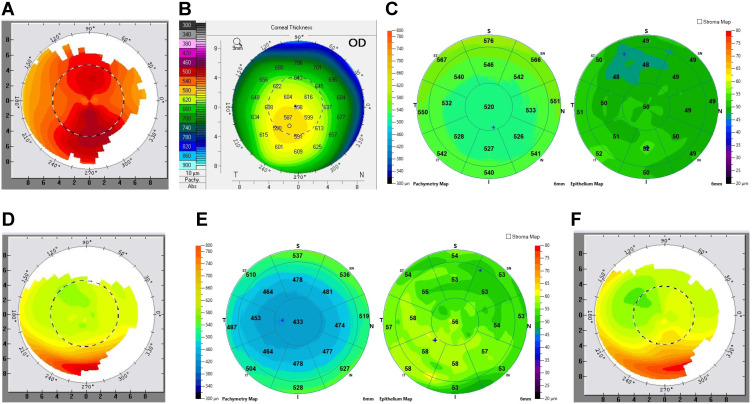
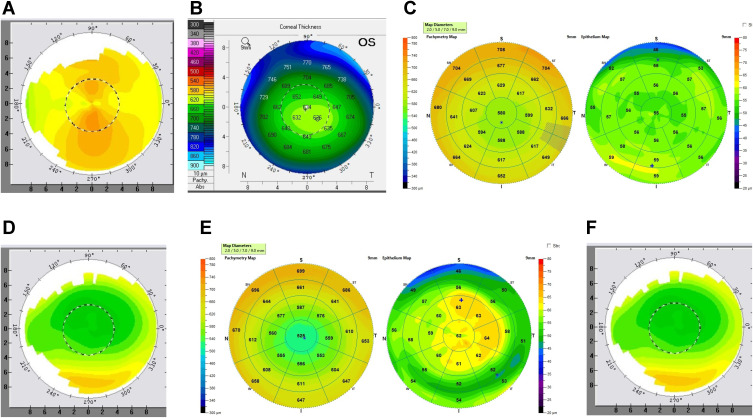
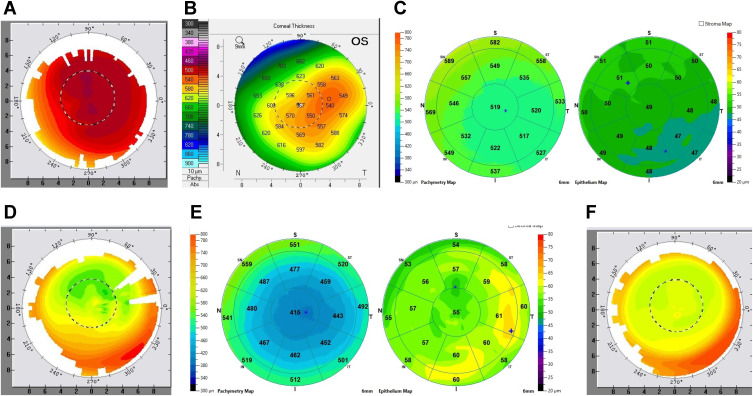
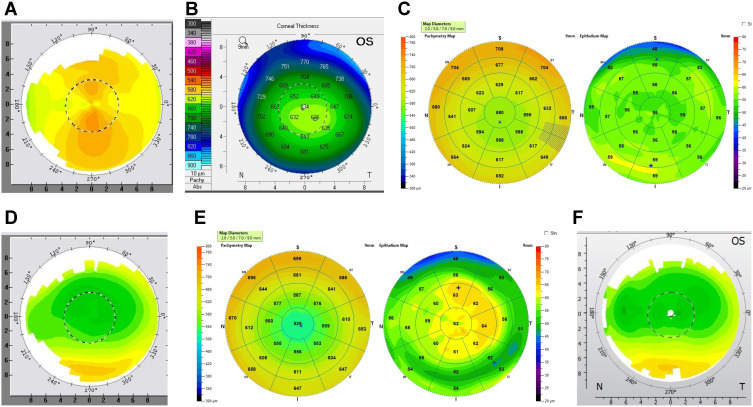
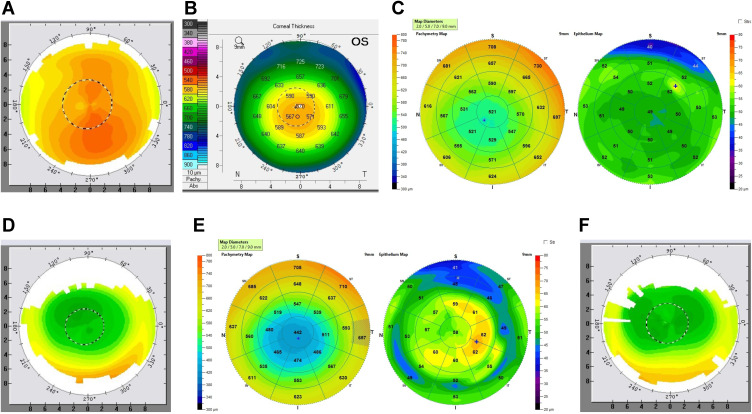
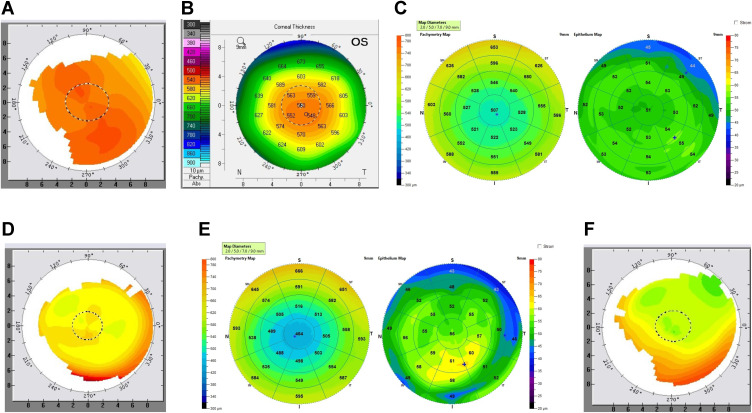
Results: Six representative cases are presented that demonstrate the biomechanical change, outcomes, and treatment. All patients demonstrated an elliptical, irregular ablation pattern on post-operative topography, lateralized the thinnest point of the cornea relative to the corneal apex on Pentacam pachymetry maps, and irregular corneal epithelial thickening at the periphery of the elliptical ablation.
Conclusion: A biomechanical change during flap creation can occur in certain types of corneas during LASIK flap creation and subsequent treatment with topographic-guided ablation leading to an irregular ablation and suboptimal refractive outcomes.
Keywords: LASIK; corneal epithelium; femtosecond laser; higher order aberration; laser ablation; laser in-situ keratomileusis.
© 2020 Motwani.
Conflict of interest statement
Dr. Motwani has received a grant from Alcon for a previous unrelated study in 2017. Dr. Motwani received non-financial support from Optovue, Inc. (loan of Optovue Avanti, clinical support in understanding analysis of data). Dr. Motwani has a patent pending on a theoretical device that could combine corneal HOA data and epithelial thickness data to achieve a more accurate refractive outcome. The author reports no other potential conflicts of interest for this work.
Figures
Similar articles
-
Analysis and Causation of All Inaccurate Outcomes After WaveLight Contoura LASIK with LYRA Protocol.Clin Ophthalmol. 2020 Nov 13;14:3841-3854. doi: 10.2147/OPTH.S267091. eCollection 2020. Clin Ophthalmol. 2020. PMID: 33223821 Free PMC article.
-
Measurement of corneal curvature change after mechanical laser in situ keratomileusis flap creation and femtosecond laser flap creation.J Cataract Refract Surg. 2008 Feb;34(2):238-42. doi: 10.1016/j.jcrs.2007.09.023. J Cataract Refract Surg. 2008. PMID: 18242446
-
Predictability of corneal flap thickness in laser in situ keratomileusis using a 200 kHz femtosecond laser.J Cataract Refract Surg. 2013 Mar;39(3):378-85. doi: 10.1016/j.jcrs.2012.10.041. Epub 2013 Jan 23. J Cataract Refract Surg. 2013. PMID: 23352500
-
Primary Topography-Guided LASIK: Refractive, Visual, and Subjective Quality of Vision Outcomes for Astigmatism ⩾2.00 Diopters.J Refract Surg. 2019 Feb 1;35(2):78-86. doi: 10.3928/1081597X-20181210-01. J Refract Surg. 2019. PMID: 30742221
-
The use of the femtosecond laser in the customization of corneal flaps in laser in situ keratomileusis.Curr Opin Ophthalmol. 2007 Jul;18(4):314-7. doi: 10.1097/ICU.0b013e3281bd88a0. Curr Opin Ophthalmol. 2007. PMID: 17568208 Review.
Cited by
-
Understanding Variable Biologic-Based Factors in Determining Laser Refractive Surgery Outcomes: A Response to the Moshirfar et al Paper [Letter].Clin Ophthalmol. 2023 Oct 18;17:3087-3088. doi: 10.2147/OPTH.S441200. eCollection 2023. Clin Ophthalmol. 2023. PMID: 37873055 Free PMC article. No abstract available.
-
Treatment of Corneal Irregularity in Radial/Astigmatic Keratotomy Patients Utilizing WaveLight Contoura.Clin Ophthalmol. 2022 Jan 11;16:111-126. doi: 10.2147/OPTH.S328050. eCollection 2022. Clin Ophthalmol. 2022. PMID: 35046636 Free PMC article.
-
Clinical Outcomes After Topography-guided Refractive Surgery in Eyes with Myopia and Astigmatism-Comparing Results with New Planning Software to Those Obtained Using the Manifest Refraction [Letter].Clin Ophthalmol. 2021 Feb 10;15:491-493. doi: 10.2147/OPTH.S298406. eCollection 2021. Clin Ophthalmol. 2021. PMID: 33603326 Free PMC article. No abstract available.
References
-
- Roberts C. Biomechanics of the cornea and wavefront-guided laser refractive surgery. J Refract Surg. 2002;18(5):S589–592. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
