

Hypercoagulopathy and Adipose Tissue Exacerbated Inflammation May Explain Higher Mortality in COVID-19 Patients With Obesity
- PMID: 32849309
- PMCID: PMC7399077
- DOI: 10.3389/fendo.2020.00530
Hypercoagulopathy and Adipose Tissue Exacerbated Inflammation May Explain Higher Mortality in COVID-19 Patients With Obesity
Abstract
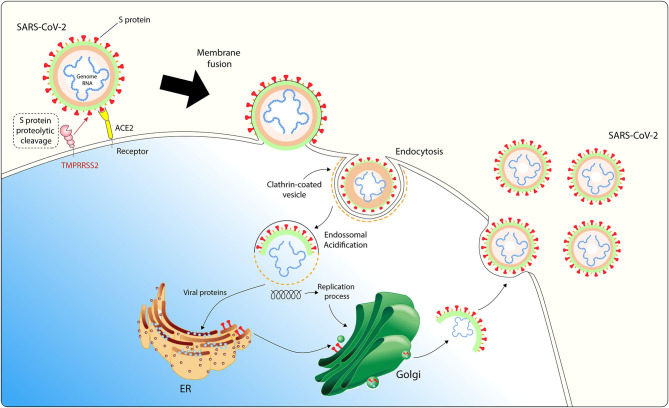
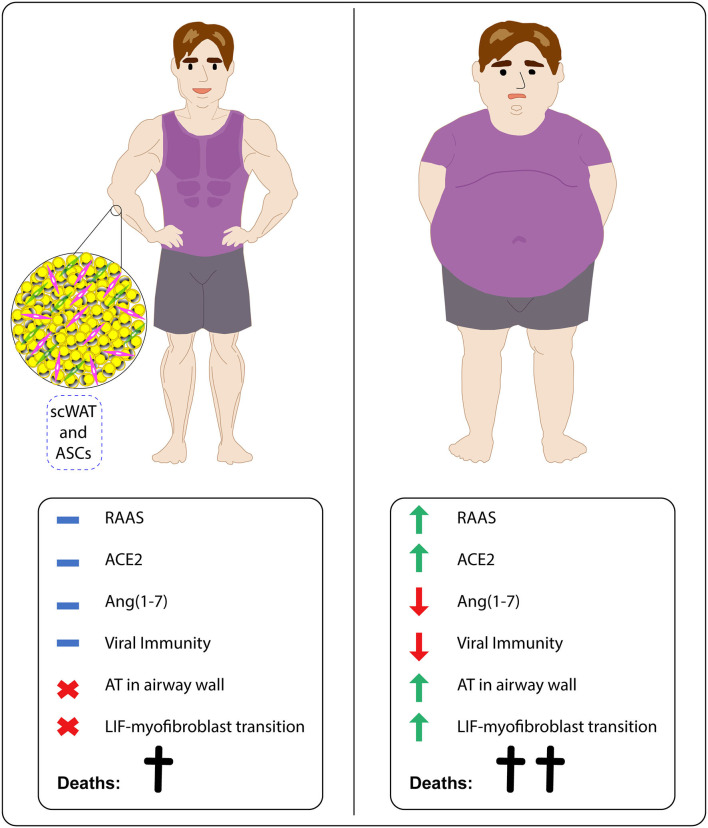
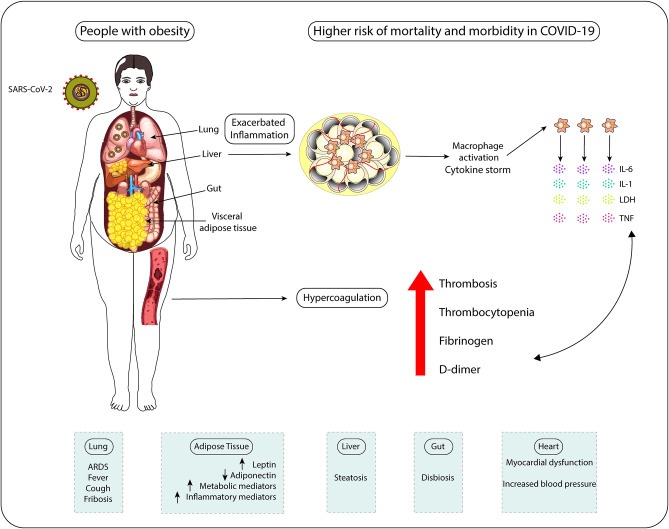
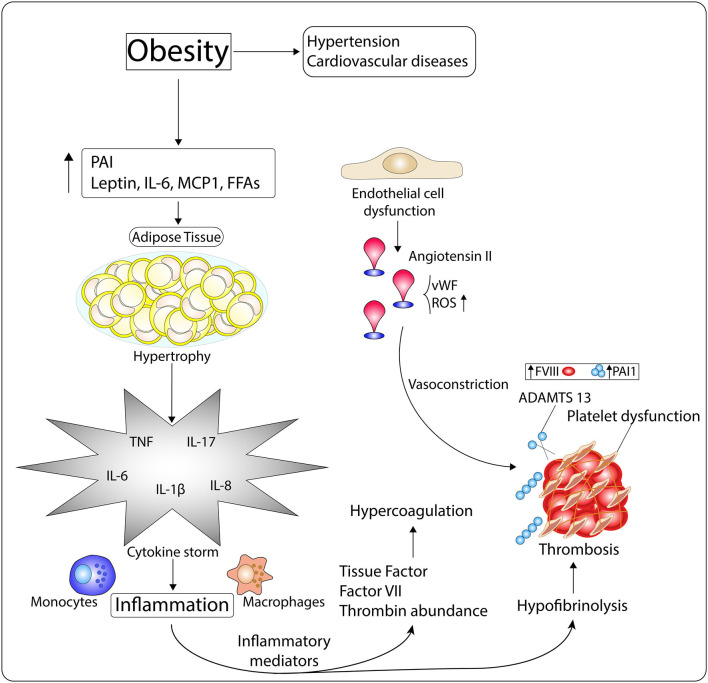
COVID-19, caused by SARS-CoV-2, is characterized by pneumonia, lymphopenia, exhausted lymphocytes and a cytokine storm. Several reports from around the world have identified obesity and severe obesity as one of the strongest risk factors for COVID-19 hospitalization and mechanical ventilation. Moreover, countries with greater obesity prevalence have a higher morbidity and mortality risk of developing serious outcomes from COVID-19. The understanding of how this increased susceptibility of the people with obesity to develop severe forms of the SARS-CoV-2 infection occurs is crucial for implementing appropriate public health and therapeutic strategies to avoid COVID-19 severe symptoms and complications in people living with obesity. We hypothesize here that increased ACE2 expression in adipose tissue displayed by people with obesity may increase SARS-CoV-2 infection and accessibility to this tissue. Individuals with obesity have increased white adipose tissue, which may act as a reservoir for a more extensive viral spread with increased shedding, immune activation and pro-inflammatory cytokine amplification. Here we discuss how obesity is related to a pro-inflammatory and metabolic dysregulation, increased SARS-CoV-2 host cell entry in adipose tissue and induction of hypercoagulopathy, leading people with obesity to develop severe forms of COVID-19 and also death. Taken together, it may be crucial to better explore the role of visceral adipose tissue in the inflammatory response to SARS-CoV-2 infection and investigate the potential therapeutic effect of using specific target anti-inflammatories (canakinumab or anakinra for IL-1β inhibition; anti-IL-6 antibodies for IL-6 inhibition), anticoagulant or anti-diabetic drugs in COVID-19 treatment of people with obesity. Defining the immunopathological changes in COVID-19 patients with obesity can provide prominent targets for drug discovery and clinical management improvement.
Keywords: ACE-2; COVID-19; Obesity; SARS-CoV-2; adipose tissue; hypercoagulopathy.
Copyright © 2020 Pasquarelli-do-Nascimento, Braz-de-Melo, Faria, Santos, Kobinger and Magalhães.
Figures
Similar articles
-
The association between obesity and poor outcome after COVID-19 indicates a potential therapeutic role for montelukast.Med Hypotheses. 2020 Oct;143:109883. doi: 10.1016/j.mehy.2020.109883. Epub 2020 May 27. Med Hypotheses. 2020. PMID: 32492562 Free PMC article.
-
SARS-CoV-2 infection and obesity: Common inflammatory and metabolic aspects.Diabetes Metab Syndr. 2020 Jul-Aug;14(4):469-471. doi: 10.1016/j.dsx.2020.04.033. Epub 2020 Apr 29. Diabetes Metab Syndr. 2020. PMID: 32387864 Free PMC article. Review.
-
COVID-19 and Obesity: Role of Ectopic Visceral and Epicardial Adipose Tissues in Myocardial Injury.Front Endocrinol (Lausanne). 2021 Aug 16;12:726967. doi: 10.3389/fendo.2021.726967. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 34484128 Free PMC article. Review.
-
Clinical characteristics and outcome in patients with combined diabetic ketoacidosis and hyperosmolar hyperglycemic state associated with COVID-19: A retrospective, hospital-based observational case series.Diabetes Res Clin Pract. 2020 Aug;166:108279. doi: 10.1016/j.diabres.2020.108279. Epub 2020 Jun 25. Diabetes Res Clin Pract. 2020. PMID: 32592843 Free PMC article.
-
From Influenza Virus to Novel Corona Virus (SARS-CoV-2)-The Contribution of Obesity.Front Endocrinol (Lausanne). 2020 Oct 6;11:556962. doi: 10.3389/fendo.2020.556962. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 33123087 Free PMC article. Review.
Cited by
-
Aging versus youth: Endocrine aspects of vulnerability for COVID-19.Rev Endocr Metab Disord. 2022 Apr;23(2):185-204. doi: 10.1007/s11154-021-09656-y. Epub 2021 Apr 16. Rev Endocr Metab Disord. 2022. PMID: 33860905 Free PMC article. Review.
-
COVID-19 and liver injury in individuals with obesity.World J Gastroenterol. 2023 Feb 14;29(6):908-916. doi: 10.3748/wjg.v29.i6.908. World J Gastroenterol. 2023. PMID: 36844135 Free PMC article. Review.
-
Reviving the mutual impact of SARS-COV-2 and obesity on patients: From morbidity to mortality.Biomed Pharmacother. 2022 Jul;151:113178. doi: 10.1016/j.biopha.2022.113178. Epub 2022 May 24. Biomed Pharmacother. 2022. PMID: 35644117 Free PMC article. Review.
-
Respiratory and nonrespiratory COVID-19 complications in patients with obesity: recent developments.J Comp Eff Res. 2022 Apr;11(5):371-381. doi: 10.2217/cer-2021-0237. Epub 2022 Jan 13. J Comp Eff Res. 2022. PMID: 35023362 Free PMC article. Review.
-
Evaluating Possible Mechanisms Linking Obesity to COVID-19: a Narrative Review.Obes Surg. 2022 May;32(5):1689-1700. doi: 10.1007/s11695-022-05933-0. Epub 2022 Feb 3. Obes Surg. 2022. PMID: 35113309 Free PMC article. Review.
References
-
- WHO Rational Use of Personal Protective Equipment for Coronavirus Disease 2019 (COVID-19). (2020). p. 1–7.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous