

Extracellular Matrix Remodeling Factors as Markers of Carotid Artery Atherosclerosis
- PMID: 32850147
- PMCID: PMC7441424
- DOI: 10.1155/2020/9036157
Extracellular Matrix Remodeling Factors as Markers of Carotid Artery Atherosclerosis
Abstract
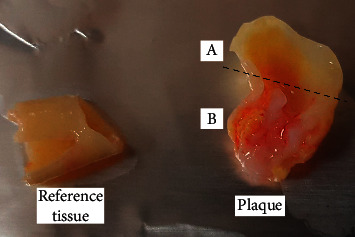
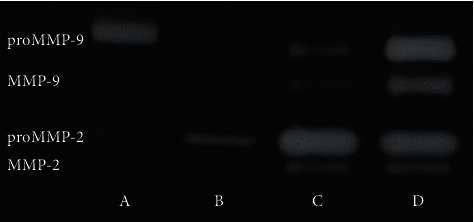
Materials and methods: 20 patients undergoing routine carotid endarterectomy and 40 healthy volunteers were enrolled in this study. MMPs activity and OPG and FN concentrations were measured in atherosclerotic plaques and nonchanged contiguous tissue after homogenization as well as in plasma from patients and reference group. The activity of MMPs was evaluated by gelatin zymography, and the concentration of OPG and FN was assessed by ELISA.
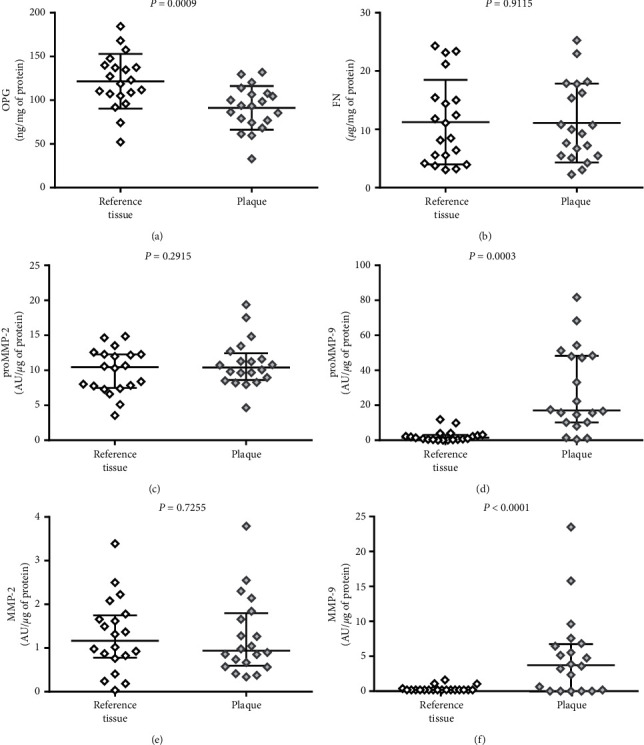
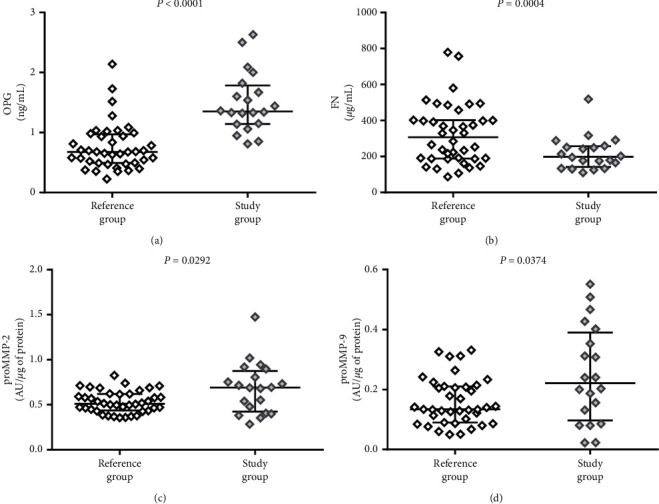
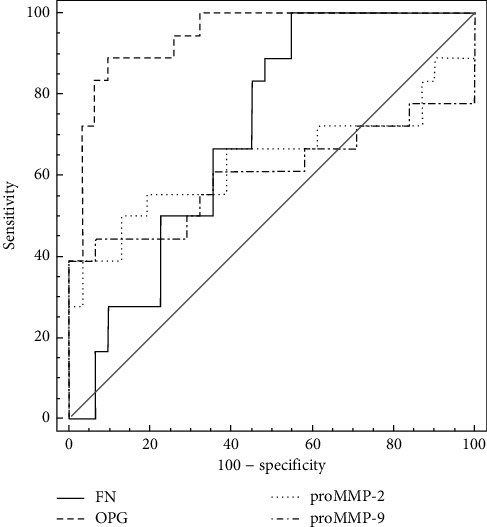
Results: OPG concentration and MMP-9 activity showed differences between plaque and nonchanged tissue; OPG was higher in adjacent tissue (P=0.0009), whereas MMP-9 was higher in plaque (proMMP-9 P=0.0003; MMP-9 P < 0.0001). The OPG plasma concentration and both MMPs plasma activity were higher in patients (OPG P < 0.001; proMMP-2 P=0.0292; and proMMP-9 P=0.0374), while FN plasma concentration was lower in patients than in the reference group (P=0.0004). The ROC curves analysis showed the highest AUC for OPG (0.943) with 85.0% sensitivity and 92.1% specificity.
Conclusions: The atherosclerotic plaque and the contiguous artery wall are biochemically different. OPG shows the highest potential to be a marker of advanced carotid atherosclerosis.
Copyright © 2020 Agnieszka Sapa-Wojciechowska et al.
Conflict of interest statement
The authors declare that there are no conflicts of interest regarding the publication of this paper.
Figures
Similar articles
-
Intraplaque MMP-8 levels are increased in asymptomatic patients with carotid plaque progression on ultrasound.Atherosclerosis. 2006 Jul;187(1):161-9. doi: 10.1016/j.atherosclerosis.2005.08.039. Epub 2005 Nov 2. Atherosclerosis. 2006. PMID: 16259988
-
Plasma Concentrations of New Biochemical Markers of Atherosclerosis in Patients with Dyslipidemia-A Pilot Study.Medicina (Kaunas). 2022 May 27;58(6):717. doi: 10.3390/medicina58060717. Medicina (Kaunas). 2022. PMID: 35743980 Free PMC article.
-
Metalloproteinases and their inhibitors are markers of plaque instability.Surgery. 2005 Mar;137(3):355-63. doi: 10.1016/j.surg.2004.10.011. Surgery. 2005. PMID: 15746792
-
[Osteoprotegerin as a marker of atherosclerosis and a prognostic factor in stroke].Postepy Hig Med Dosw (Online). 2015 Dec 31;69:1505-11. Postepy Hig Med Dosw (Online). 2015. PMID: 27259222 Review. Polish.
-
MMP-9 and/or TIMP as predictors of ischaemic stroke in patients with symptomatic and asymptomatic atherosclerotic stenosis of carotid artery treated by stenting or endarterectomy - A review.Neurol Neurochir Pol. 2018 Sep-Oct;52(5):555-561. doi: 10.1016/j.pjnns.2018.05.005. Epub 2018 May 30. Neurol Neurochir Pol. 2018. PMID: 29875068
Cited by
-
Telocytes promote hepatocellular carcinoma by activating the ERK signaling pathway and miR-942-3p/MMP9 axis.Cell Death Discov. 2021 Aug 10;7(1):209. doi: 10.1038/s41420-021-00592-z. Cell Death Discov. 2021. PMID: 34376644 Free PMC article.
-
The Genetics of Coronary Artery Disease: A Vascular Perspective.Cells. 2023 Sep 8;12(18):2232. doi: 10.3390/cells12182232. Cells. 2023. PMID: 37759455 Free PMC article. Review.
-
Non-Coding RNAs in Regulating Plaque Progression and Remodeling of Extracellular Matrix in Atherosclerosis.Int J Mol Sci. 2022 Nov 8;23(22):13731. doi: 10.3390/ijms232213731. Int J Mol Sci. 2022. PMID: 36430208 Free PMC article. Review.
References
-
- Naylor A. R., Ricco J. B., De Borst G. J., et al. Editor’s choice-management of atherosclerotic carotid and vertebral artery disease: 2017 clinical practice guidelines of the european society for vascular surgery (ESVS) European Journal of Vascular and Endovascular Surgery. 2018;55(1):3–81. doi: 10.1016/j.ejvs.2017.06.021. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous