

Local uterine resection with Bakri balloon placement in placenta accreta spectrum disorders
- PMID: 32850185
- PMCID: PMC7406901
- DOI: 10.4274/tjod.galenos.2020.82652
Local uterine resection with Bakri balloon placement in placenta accreta spectrum disorders
Abstract
Objective: Placenta accreta spectrum (PAS) is a potentially life-threatening condition characterized by the abnormal adherence of the placenta to the implantation site. We sought to evaluate the efficacy, surgical feasibility, risks, and advantages of local uterine resection in cases complicated with PAS.
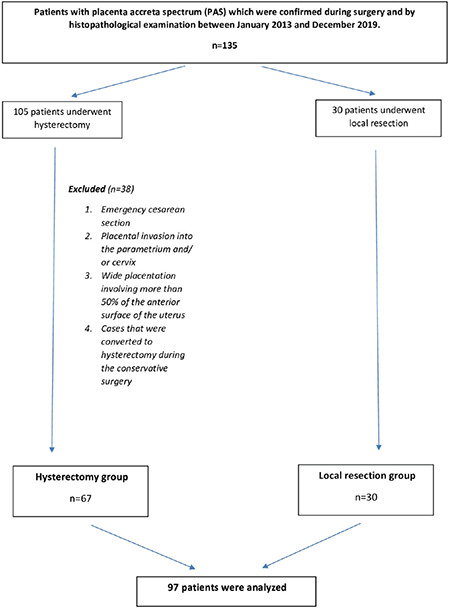
Materials and methods: This study included 97 patients with PAS, which was confirmed during surgery and by histopathological examination between January 2013 and December 2019. The patients were divided into two groups based on operative approach. The study population (local resection group) consisted of 30 cases in whom total resection of adherent placenta and myometrium was performed, whereas the control group (hysterectomy group) of 67 cesarean hysterectomy cases.
Results: Patients who underwent hysterectomy had significantly more bleeding than the local resection group (1180±160 mL vs 877±484 mL; p=0.002). The mean number of transfused packed red blood cells (pRBCs) was greater in the hysterectomy group (4.5±2.3) than in the local resection group (2.6±3.1; p=0.001). Transfusion rate of four and/or more pRBCs was 67.2% in the hysterectomy group and 33.3% in the local resection group, which indicated a statistically significant difference (p=0.002). Of patients, 29.6% required intensive care unit in the hysterectomy group and 6.7% in the local resection group (p=0.023).
Conclusion: Local resection can be performed safely in selected PAS cases. In these cases, using a standardized protocol in terms of patient selection and surgical procedure will reduce morbidity and mortality.
Keywords: Conservative technique; local resection; placenta accreta; placenta accreta spectrum; placenta percreta.
©Copyright 2020 by Turkish Society of Obstetrics and Gynecology | Turkish Journal of Obstetrics and Gynecology published by Galenos Publishing House.
Figures
References
-
- D’antonio F, Iacovella C, Bhide A. Prenatal identification of invasive placentation using ultrasound: Systematic review and meta‐analysis. Ultrasound Obstet Gynecol. 2013;42:509–17. - PubMed
-
- Irving F. A study of placenta accreta. Surg Gynecol Obstet. 1937;64:178–200.
-
- Jauniaux E, Jurkovic D. Placenta accreta: pathogenesis of a 20th century iatrogenic uterine disease. Placenta. 2012;33:244–51. - PubMed
-
- Bowman ZS, Eller AG, Bardsley TR, Greene T, Varner MW, Silver RM. Risk factors for placenta accreta: A large prospective cohort. Am J Perinatol. 2014;31:799–804. - PubMed
-
- Jauniaux E, Collins SL, Jurkovic D, Burton GJ. Accreta placentation: a systematic review of prenatal ultrasound imaging and grading of villous invasiveness. Am J Obstet Gynecol. 2016;215:712–21. - PubMed
LinkOut - more resources
Full Text Sources