

Positive Chest CT Features in Patients With COVID-19 Pneumonia and Negative Real-Time Polymerase Chain Reaction Test
- PMID: 32850265
- PMCID: PMC7444987
- DOI: 10.7759/cureus.9942
Positive Chest CT Features in Patients With COVID-19 Pneumonia and Negative Real-Time Polymerase Chain Reaction Test
Abstract
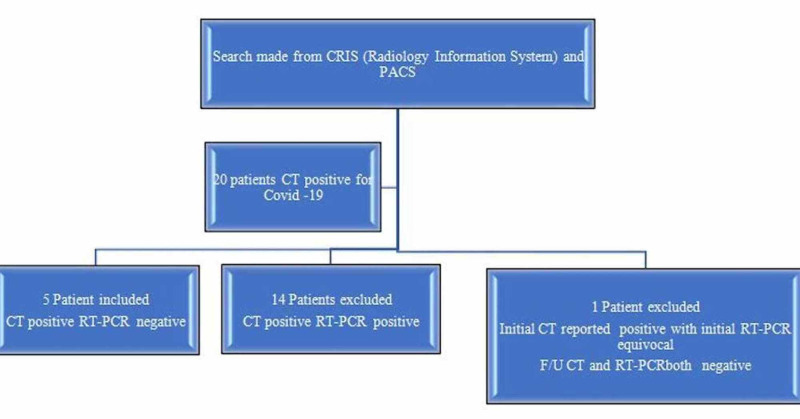
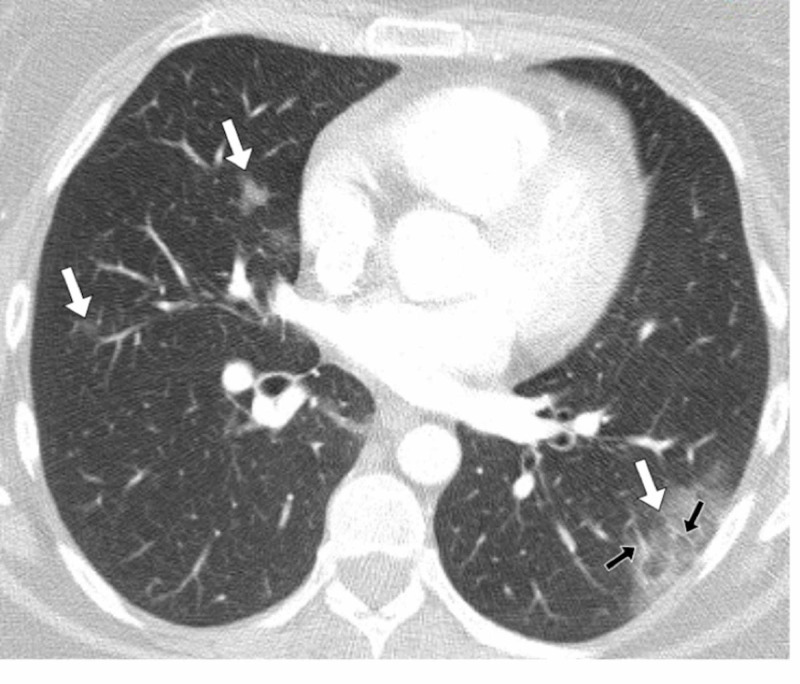
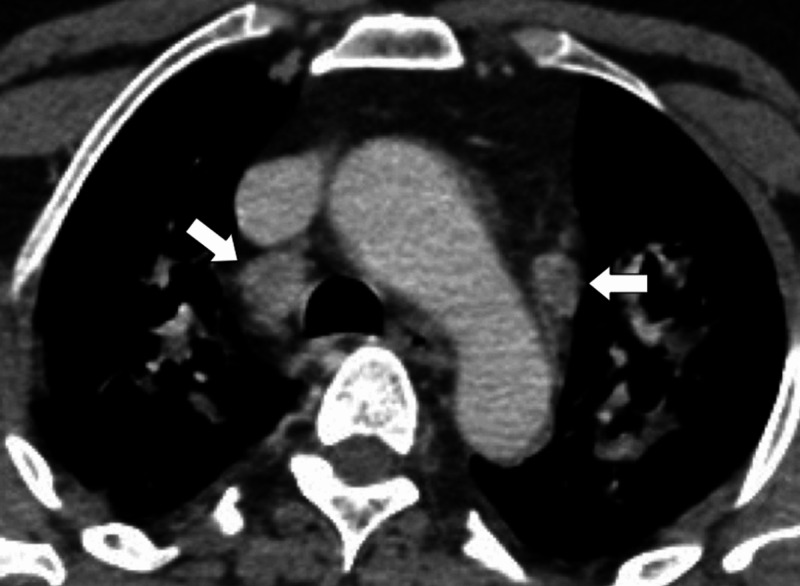
Objectives Clinically suspicious novel coronavirus (COVID-19) lung pneumonia can be observed typically on computed tomography (CT) chest scans even in patients with a negative real-time polymerase chain reaction (RT-PCR) test. The purpose of the study was to describe the CT imaging findings of five patients with negative RT-PCR results on initial and repeated testing but a high radiological suspicion of COVID-19 pneumonia. Methods Out of 19 clinically and/or radiologically diagnosed COVID-19 patients from our institution, five patients were selected for our study who had typical findings of COVID-19 on CT scan despite two negative RT-PCR results. Two district general hospital radiologists reviewed the chest CT images without prior knowledge of the RT-PCR test results. Scans were analyzed for the density of opacification and the distribution of disease. Results Out of 19 patients, five (26%) had initial negative RT-PCR test findings but positive CT chest features consistent with COVID-19. All patients had typical CT imaging findings of COVID-19. These included one patient with purely ground-glass opacities (GGO) and four patients with mixed GGO and consolidation. The typical distribution of parenchymal involvement was bilateral, posterior, and peripheral. Of the five patients with negative RT-PCR and positive CT findings, the range of CT severity score was 5 to 14. The median score, seen in three patients, was a score of 5, which corresponded to mild disease. One patient had a score of 8, corresponding to moderate disease, and one patient had severe disease with a score of 14. Conclusion Lung parenchymal changes related to COVID-19 can be seen on chest CT clearly despite repeated RT-PCR negative results.
Keywords: 2019-ncov; chest ct; covid-19; novel coronavirus; rt-pcr; sars-cov-2.
Copyright © 2020, Pakdemirli et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures






Similar articles
-
Clinical Features and Chest CT Manifestations of Coronavirus Disease 2019 (COVID-19) in a Single-Center Study in Shanghai, China.AJR Am J Roentgenol. 2020 Jul;215(1):121-126. doi: 10.2214/AJR.20.22959. Epub 2020 Mar 14. AJR Am J Roentgenol. 2020. PMID: 32174128
-
Diagnostic accuracy and false-positive rate of chest CT as compared to RT-PCR in coronavirus disease 2019 (COVID-19) pneumonia: A prospective cohort of 612 cases from India and review of literature.Indian J Radiol Imaging. 2021 Jan;31(Suppl 1):S161-S169. doi: 10.4103/ijri.IJRI_377_20. Epub 2021 Jan 23. Indian J Radiol Imaging. 2021. PMID: 33814777 Free PMC article.
-
Clinical Application of Chest Computed Tomography (CT) in Detection and Characterization of Coronavirus (Covid-19) Pneumonia in Adults.J Digit Imaging. 2021 Apr;34(2):273-283. doi: 10.1007/s10278-021-00426-5. Epub 2021 Feb 9. J Digit Imaging. 2021. PMID: 33565000 Free PMC article.
-
Chest CT features of coronavirus disease 2019 (COVID-19) pneumonia: key points for radiologists.Radiol Med. 2020 Jul;125(7):636-646. doi: 10.1007/s11547-020-01237-4. Epub 2020 Jun 4. Radiol Med. 2020. PMID: 32500509 Free PMC article. Review.
-
Predictors of the chest CT score in COVID-19 patients: a cross-sectional study.Virol J. 2021 Nov 18;18(1):225. doi: 10.1186/s12985-021-01699-6. Virol J. 2021. PMID: 34794467 Free PMC article. Review.
Cited by
-
High-Resolution CT Chest Findings in Suspected COVID-19 Pneumonia Patients With Negative Real-Time Polymerase Chain Reaction Assay.Cureus. 2021 Mar 21;13(3):e14023. doi: 10.7759/cureus.14023. Cureus. 2021. PMID: 33889463 Free PMC article.
-
Clinical findings, viral load, and outcomes of COVID-19: Comparison of patients with negative and positive initial chest computed tomography.PLoS One. 2022 Mar 3;17(3):e0264711. doi: 10.1371/journal.pone.0264711. eCollection 2022. PLoS One. 2022. PMID: 35239734 Free PMC article.
-
The AndroCoV Clinical Scoring for COVID-19 Diagnosis: A Prompt, Feasible, Costless, and Highly Sensitive Diagnostic Tool for COVID-19 Based on a 1757-Patient Cohort.Cureus. 2021 Jan 7;13(1):e12565. doi: 10.7759/cureus.12565. Cureus. 2021. PMID: 33437562 Free PMC article.
-
Role of High Resolution Computed Tomography chest in the diagnosis and evaluation of COVID -19 patients -A systematic review and meta-analysis.Eur J Radiol Open. 2021;8:100350. doi: 10.1016/j.ejro.2021.100350. Epub 2021 May 13. Eur J Radiol Open. 2021. PMID: 34007865 Free PMC article.
-
The Efficacy of Tracheotomy for Covid-19 Pneumonia: Impacts on Survival and Prognostic Factors.Indian J Otolaryngol Head Neck Surg. 2022 Oct;74(Suppl 2):3016-3021. doi: 10.1007/s12070-021-02717-3. Epub 2021 Jul 6. Indian J Otolaryngol Head Neck Surg. 2022. PMID: 34249667 Free PMC article.
References
-
- Chest CT findings in 2019 novel coronavirus (2019-nCoV) infections from Wuhan, China: key points for the radiologist. Kanne JP. https://pubs.rsna.org/doi/10.1148/radiol.2020200241 Radiology. 2020;295:0. - PMC - PubMed
-
- World Health Organization (WHO) Europe. WHO announces COVID-19 outbreak a pandemic. [Jun;2020 ];https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus... 2020 :2020–2023.
LinkOut - more resources
Full Text Sources
Miscellaneous