

Ruxolitinib Rapidly Reduces Acute Respiratory Distress Syndrome in COVID-19 Disease. Analysis of Data Collection From RESPIRE Protocol
- PMID: 32850921
- PMCID: PMC7417512
- DOI: 10.3389/fmed.2020.00466
Ruxolitinib Rapidly Reduces Acute Respiratory Distress Syndrome in COVID-19 Disease. Analysis of Data Collection From RESPIRE Protocol
Abstract
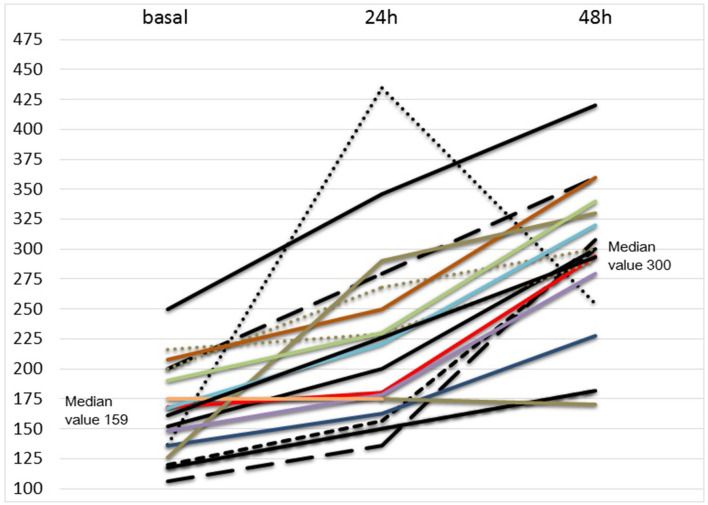
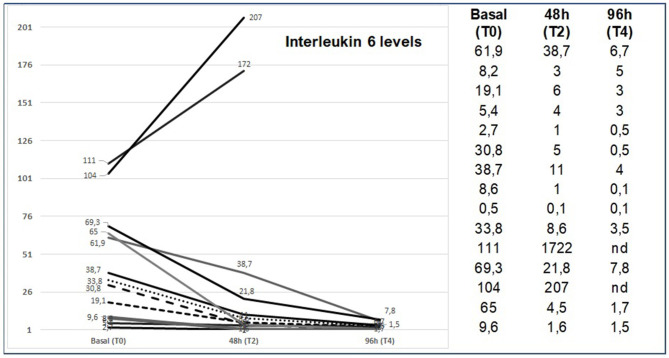
Background: The Coronavirus disease (COVID-19) pandemic is causing millions of infections and hundreds of thousands of deaths worldwide. Cumulative clinical and laboratory evidence suggest that a subset of patients with severe COVID-19 may develop a cytokine storm syndrome during the course of the disease, with severe respiratory impairment requiring ventilatory support. One field of research nowadays is to identify and treat viral-induced hyperinflammation with drugs used in other clinical conditions characterized by an hyperinflammation status. These drugs might help to reduce COVID19 mortality. Methods: Ruxolitinib, a JAK1 and JAK2 inhibitor, has been successfully used to treat severe immune-mediated diseases, such as graft vs. host disease and Hemophagocytic lymphohistiocytosis. We used ruxolitinib in 18 patients with clinically progressive COVID-19 related acute respiratory distress syndrome, with a primary endpoint to rapidly reduce the degree of respiratory impairment and as a secondary endpoint to rapidly restore the PaO2/FiO2 ratio, as an evaluation of clinical status, and monitoring of drug related Adverse Events. Parameters of inflammation responses and organ functions were assessed and monitored. The treatment plan was ruxolitinib 20 mg bid for the first 48 h and subsequent two-step de-escalation at 10 mg bid and 5 mg bid for a maximum of 14 days of treatment. Results: Our data collection shows a rapid clinical response with no evolution from non-invasive ventilation to mechanical ventilation in 16/18 patients and no response in two patients (overall response rate-ORR 89%). Already after 48 h of ruxolitinib treatment 16/18 patients showed evident clinical improvement, and after 7 days of treatment 11/18 patients showed fully recovered respiratory function (pO2 > 98% in spontaneous breathing), 4/18 patients had minimal oxygen requirement (2-4 L/m), 1/18 patient showed stable disease, and 2/18 patient showed progressive disease. After 14 days, 16/18 patients showed complete recovery of respiratory function (ORR 89%). Compliance to ruxolitinib planned treatment was 100% and no serious adverse event was recorded. In our case series of 18 critically ill patients with COVID-19 and ARDS, administration of ruxolitinib resulted in a clinical improvement that concurred to modify the standard course of disease. Ruxolitinib can be a therapeutic option for patients with respiratory insufficiency in COVID-19 related ARDS. RESPIRE Study (Ruxolitinib for the treatment of acute rESPIratory distREss syndrome, ClinicalTrials.gov Identifier: NCT04361903).
Keywords: COVID-19; ICU; respiratory distress syndrome; ruxolitinib; treatment.
Copyright © 2020 Capochiani, Frediani, Iervasi, Paolicchi, Sani, Roncucci, Cuccaro, Franchi, Simonetti, Carrara, Bertaggia, Nasso, Riccioni, Scolletta, Valente, Conticini, Gozzetti and Bocchia.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous