

Expanding and validating the biomarkers for mitochondrial diseases
- PMID: 32851462
- PMCID: PMC7524861
- DOI: 10.1007/s00109-020-01967-y
Expanding and validating the biomarkers for mitochondrial diseases
Abstract
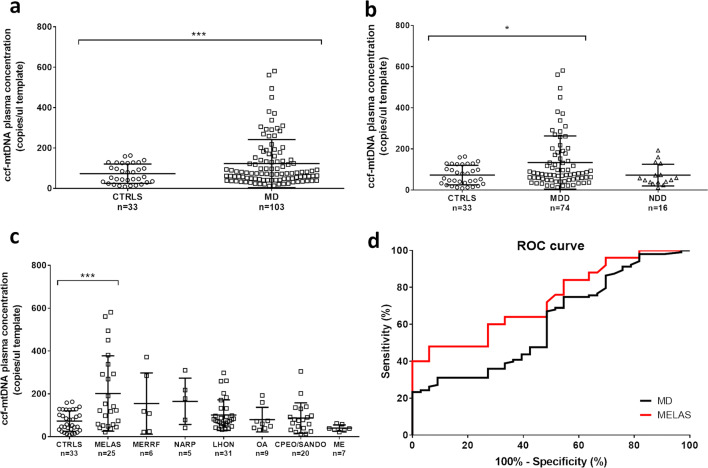
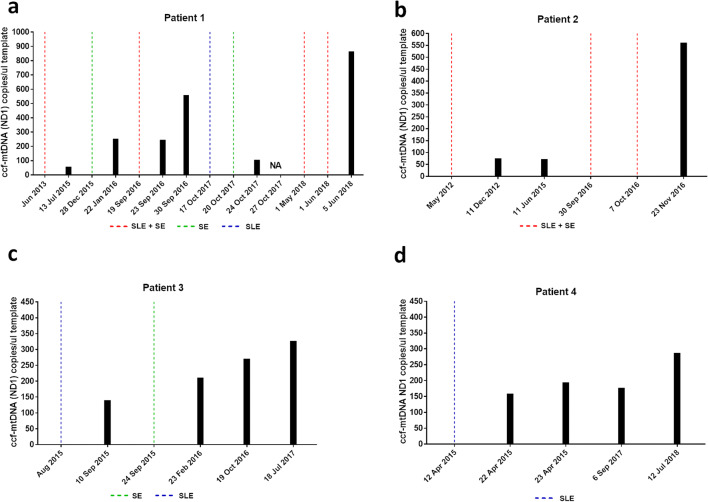
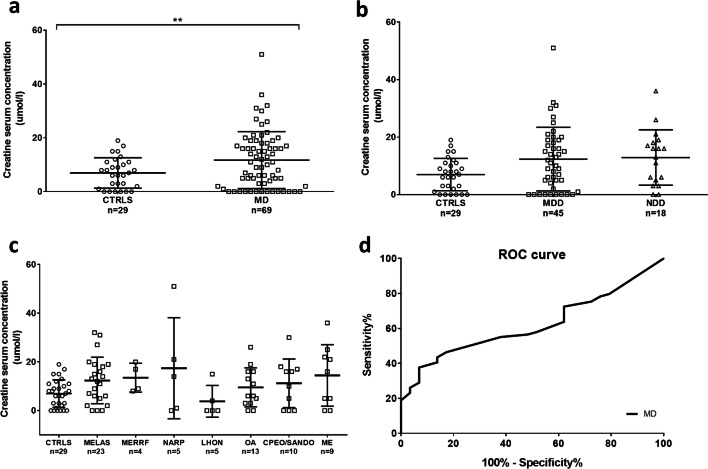
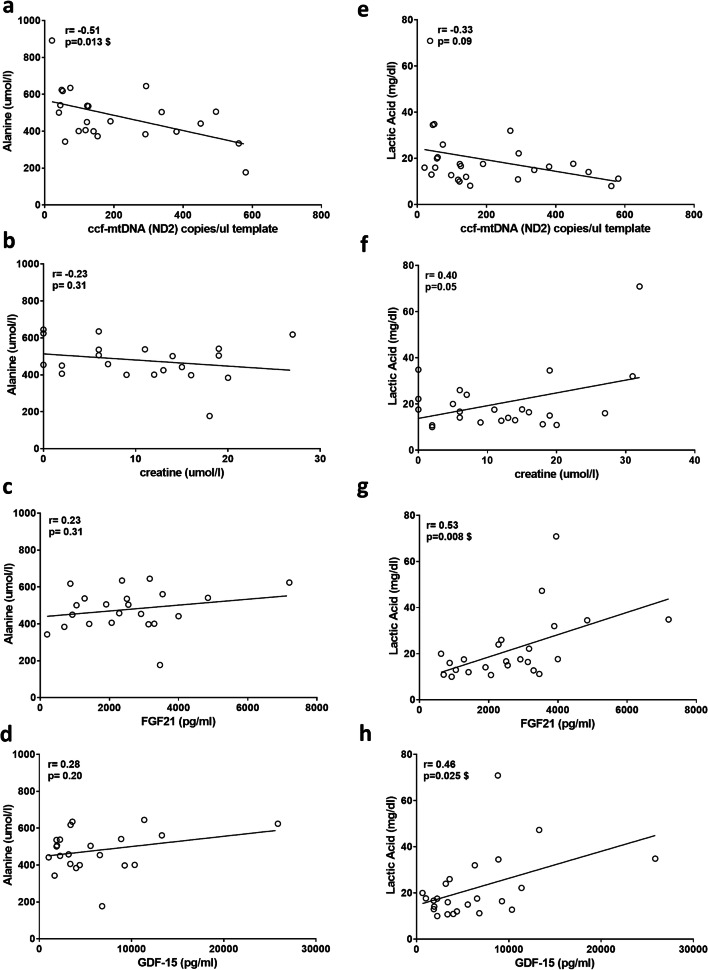
Mitochondrial diseases are highly heterogeneous metabolic disorders caused by genetic alterations in the mitochondrial DNA (mtDNA) or in the nuclear genome. In this study, we investigated a panel of blood biomarkers in a cohort of 123 mitochondrial patients, with prominent neurological and muscular manifestations. These biomarkers included creatine, fibroblast growth factor 21 (FGF21) and growth/differentiation factor 15 (GDF-15), and the novel cell free circulating-mtDNA (ccf-mtDNA). All biomarkers were significantly increased in the patient group. After stratification by the specific phenotypes, ccf-mtDNA was significantly increased in the Mitochondrial Encephalomyopathy Lactic Acidosis Stroke-like episodes syndrome (MELAS) group, and FGF21 and GDF-15 were significantly elevated in patients with MELAS and Myoclonic Epilepsy Ragged Red Fibers syndrome. On the contrary, in our cohort, creatine was not associated to a specific clinical phenotype. Longitudinal assessment in four MELAS patients showed increased levels of ccf-mtDNA in relation to acute events (stroke-like episodes/status epilepticus) or progression of neurodegeneration. Our results confirm the association of FGF21 and GDF-15 with mitochondrial translation defects due to tRNA mutations. Most notably, the novel ccf-mtDNA was strongly associated with MELAS and may be used for monitoring the disease course or to evaluate the efficacy of therapies, especially in the acute phase. KEY MESSAGES: • FGF21/GDF15 efficiently identifies mitochondrial diseases due to mutations in tRNA genes. • The novel ccf-mtDNA is associated with MELAS and increases during acute events. • Creatine only discriminates severe mitochondrial patients. • FGF21, GDF-15, and ccf-mtDNA are possibly useful for monitoring therapy efficacy.
Keywords: Biomarkers; Cell free circulating-mtDNA; Creatine; FGF21; GDF-15; Mitochondrial diseases.
Conflict of interest statement
AM, VDD, MR, LDV, MC, and MLV have no conflict of interest.
CLM has received speaker honoraria and travel reimbursements for meetings from the Santhera Pharmaceuticals, outside the present study.
VC is a consultant and runs clinical trials for Santhera Pharmaceuticals, Gensight Biologics, and Stealth BioTherapeutics, receiving speaker honoraria and traveling reimbursements, outside the present study; VC also received an unrestricted research grant support from Stealth BioTherapeutics unrelated to the present study.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
