

Spontaneous visual exploration during locomotion in patients with phobic postural vertigo
- PMID: 32852578
- PMCID: PMC7718196
- DOI: 10.1007/s00415-020-10151-8
Spontaneous visual exploration during locomotion in patients with phobic postural vertigo
Abstract
Background: Earlier studies on stance and gait with posturographic and EMG-recordings and automatic gait analysis in patients with phobic postural vertigo (PPV) or visual height intolerance (vHI) revealed similar patterns of body stiffening with muscle co-contraction and a slow, cautious gait. Visual exploration in vHI patients was characterized by a freezing of gaze-in-space when standing and reduced horizontal eye and head movements during locomotion.
Objective: Based on the findings in vHI patients, the current study was performed with a focus on visual control of locomotion in patients with PPV while walking along a crowded hospital hallway.
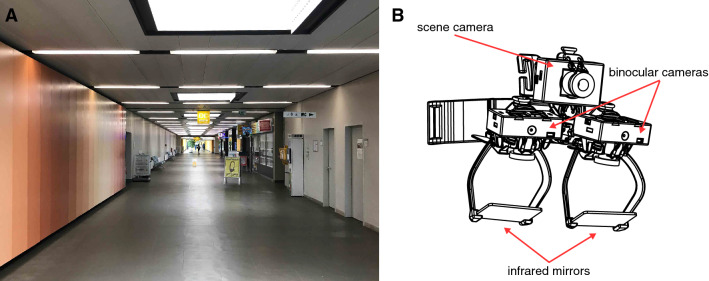
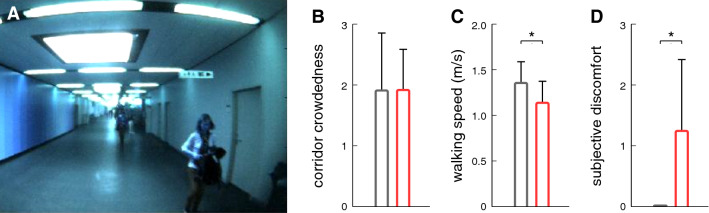
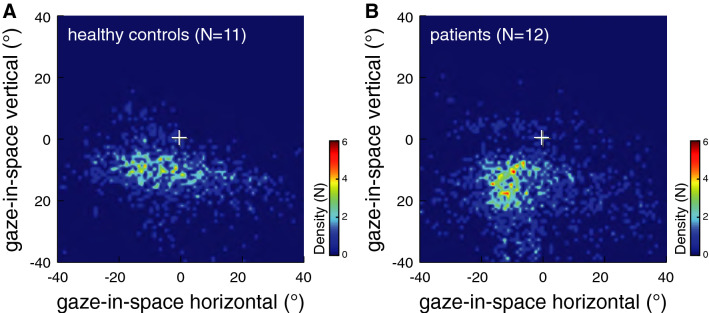
Methods: Twelve patients with PPV and eleven controls were recruited. Participants wore a mobile infrared video eye-tracking system that continuously measured eye-in-head movements in the horizontal and vertical planes and head orientation and motion in the yaw, pitch, and roll planes. Visual exploration behavior of participants was recorded at the individually preferred speed for a total walking distance of 200 m. Gaze-in-space directions were determined by combining eye-in-head and head-in-space orientation. Walking speeds were calculated based on the trial duration and the total distance traversed. Participants were asked to rate their feelings of discomfort during the walk on a 4-point numeric rating scale. The examiners rated the crowdedness of the hospital hallway on a 4-point numeric rating scale.
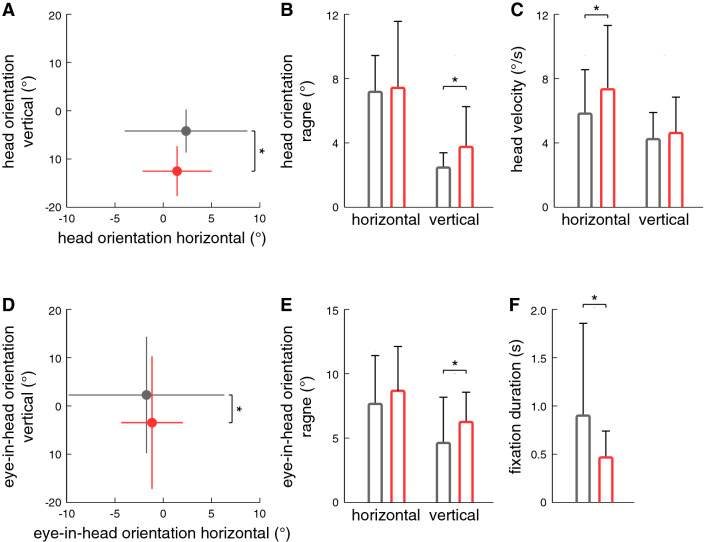
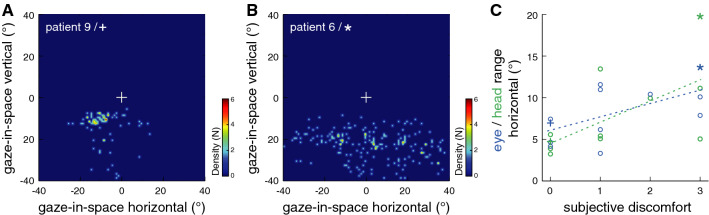
Results: The major results of visual exploration behavior in patients with PPV in comparison to healthy controls were: eye and head positions were directed more downward in the vertical plane towards the ground ahead with increased frequency of large amplitude vertical orientation movements towards the destination, the end of the ground straight ahead. The self-adjusted speed of locomotion was significantly lower in PPV. Particularly those patients that reported high levels of discomfort exhibited a specific visual exploration of their horizontal surroundings. The durations of fixating targets in the visual surroundings were significantly shorter as compared to controls.
Conclusion: Gaze control of locomotion in patients with PPV is characterized by a preferred deviation of gaze more downward and by horizontal explorations for suitable auxiliary means for potential postural support in order to prevent impending falls. These eye movements have shorter durations of fixation as compared to healthy controls and patients with vHI. Finally, the pathological alterations in eye-head coordination during locomotion correlate with a higher level of discomfort and anxiety about falling.
Keywords: Eye movements; Functional dizziness; Head movements; Phobic postural vertigo; Visual exploration.
Conflict of interest statement
On behalf of all authors, the corresponding author states that there is no conflict of interest. S. Bardins is a shareholder of EyeSeeTec GmbH, manufacturer of the eye-tracking equipment used in the study.
Figures
Similar articles
-
Visual exploration during locomotion limited by fear of heights.PLoS One. 2014 Aug 28;9(8):e105906. doi: 10.1371/journal.pone.0105906. eCollection 2014. PLoS One. 2014. PMID: 25165822 Free PMC article.
-
Fear of heights freezes gaze to the horizon.J Vestib Res. 2014;24(5-6):433-41. doi: 10.3233/VES-140529. J Vestib Res. 2014. PMID: 25564086 Clinical Trial.
-
Acrophobia impairs visual exploration and balance during standing and walking.Ann N Y Acad Sci. 2015 Apr;1343:37-48. doi: 10.1111/nyas.12692. Epub 2015 Feb 26. Ann N Y Acad Sci. 2015. PMID: 25722015 Review.
-
[How acrophobia impairs visual exploration and gait].Nervenarzt. 2013 Oct;84(10):1233-7. doi: 10.1007/s00115-013-3905-6. Nervenarzt. 2013. PMID: 24057067 German.
-
Acrophobia and visual height intolerance: advances in epidemiology and mechanisms.J Neurol. 2020 Dec;267(Suppl 1):231-240. doi: 10.1007/s00415-020-09805-4. Epub 2020 May 22. J Neurol. 2020. PMID: 32444982 Free PMC article. Review.
Cited by
-
Neurological update: neuro-otology 2023.J Neurol. 2023 Dec;270(12):6170-6192. doi: 10.1007/s00415-023-11922-9. Epub 2023 Aug 17. J Neurol. 2023. PMID: 37592138 Free PMC article.
-
Central vestibular networking for sensorimotor control, cognition, and emotion.Curr Opin Neurol. 2024 Feb 1;37(1):74-82. doi: 10.1097/WCO.0000000000001233. Epub 2023 Nov 30. Curr Opin Neurol. 2024. PMID: 38032266 Free PMC article. Review.
-
Impact of proprioceptive cervical dizziness in chronic neck pain syndromes on gait and stance during active head-turn challenges.J Neurol. 2024 Dec;271(12):7460-7470. doi: 10.1007/s00415-024-12711-8. Epub 2024 Oct 15. J Neurol. 2024. PMID: 39404783 Free PMC article.
References
-
- Brandt T. Phobic postural vertigo. Neurology. 1996;46:1515–1519. - PubMed
-
- Dieterich M, Staab JP, Brandt T. Functional (psychogenic) dizziness. Handb Clin Neurol. 2016;139:447–468. - PubMed
-
- Dieterich M, Staab JP. Functional dizziness: from phobic postural vertigo and chronic subjective dizziness to persistent postural-perceptual dizziness. Curr Opin Neurol. 2017;30:107–113. - PubMed
-
- Brandt T, Dieterich M. The dizzy patient: don’t forget disorders of the central vestibular system. Nat Rev Neurol. 2017;13:352–362. - PubMed
-
- Krafczyk S, Schlamp V, Dieterich M, Haberhauer P, Brandt T. Increased body sway at 3.5–8 Hz in patients with phobic postural vertigo. Neurosci Lett. 1999;259:149–152. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
