

Comparison of a novel Compressed SENSE accelerated 3D modified relaxation-enhanced angiography without contrast and triggering with CE-MRA in imaging of the thoracic aorta
- PMID: 32852711
- PMCID: PMC7878228
- DOI: 10.1007/s10554-020-01979-2
Comparison of a novel Compressed SENSE accelerated 3D modified relaxation-enhanced angiography without contrast and triggering with CE-MRA in imaging of the thoracic aorta
Abstract
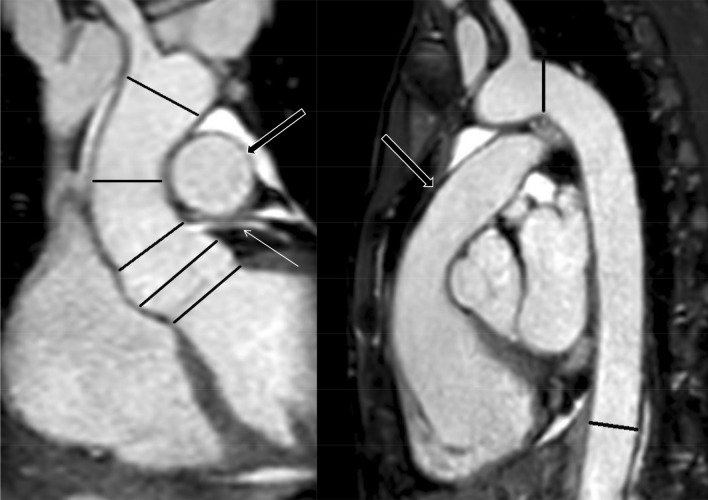
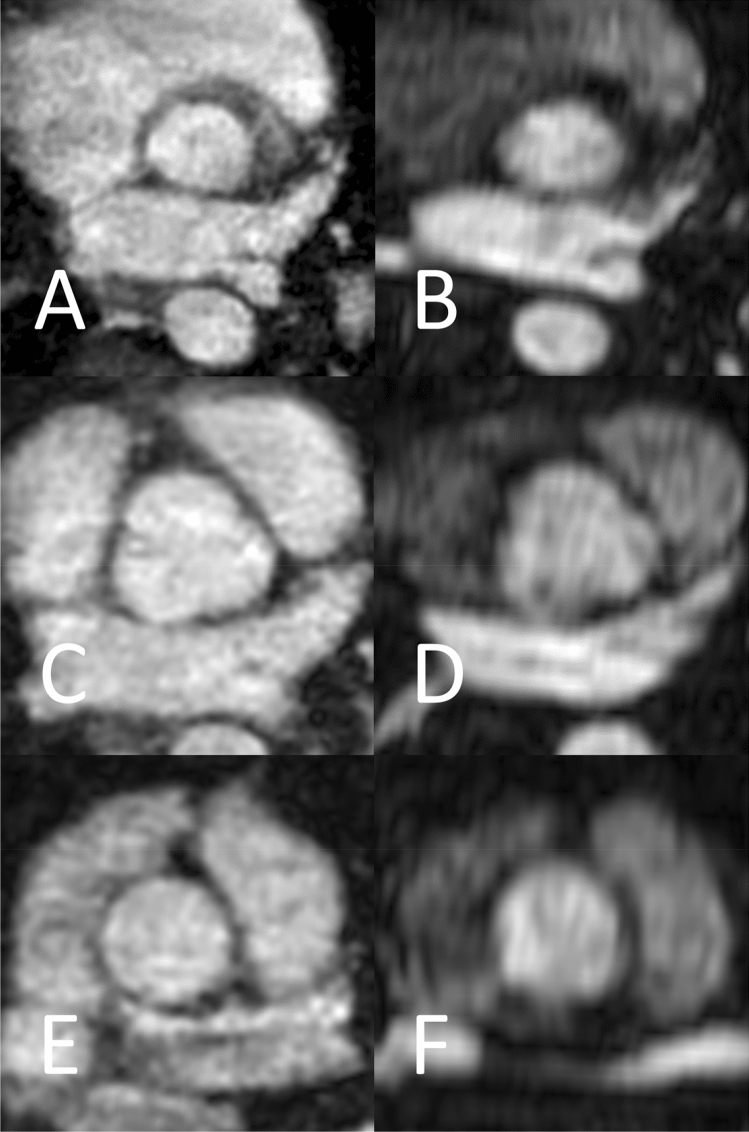
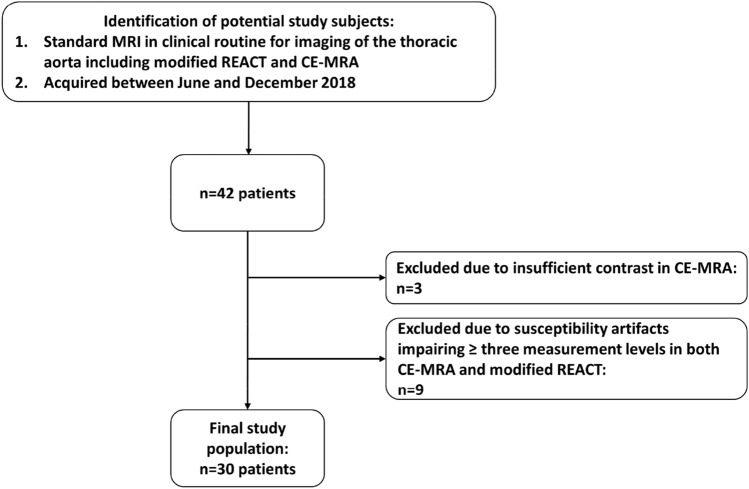
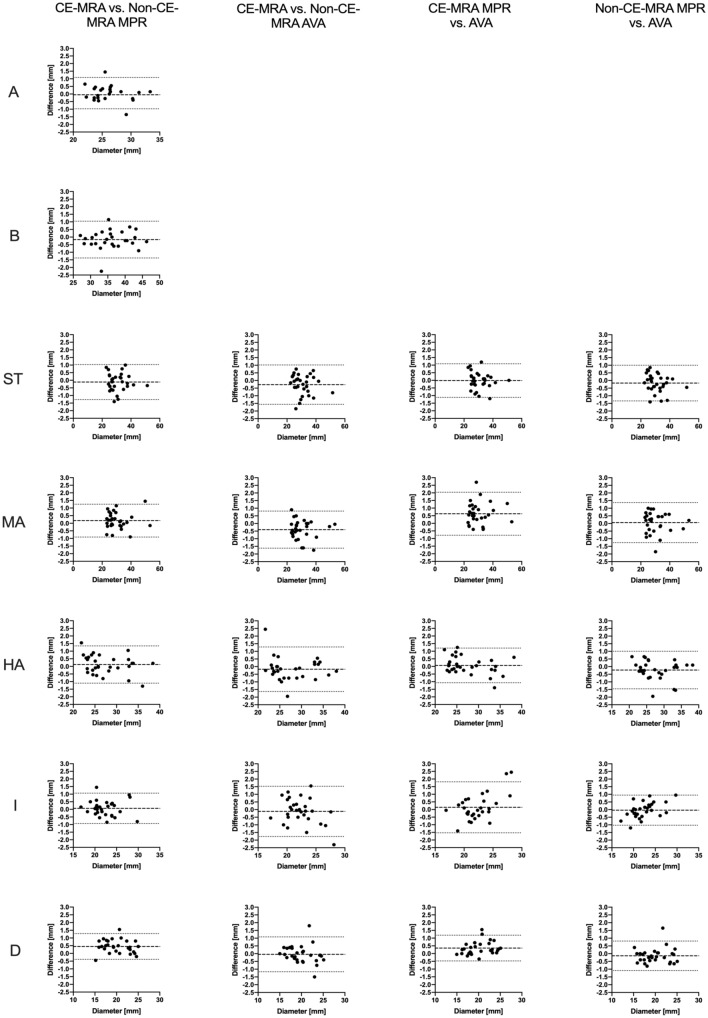
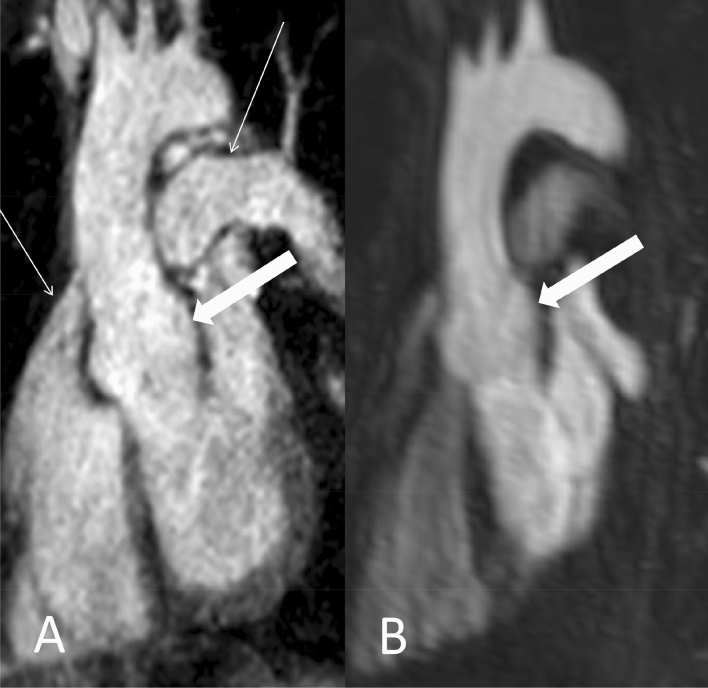
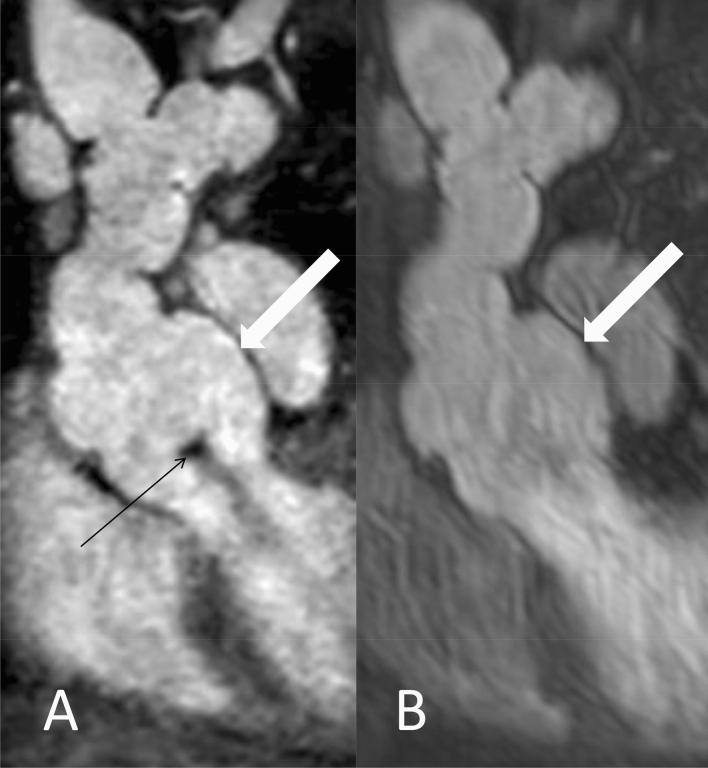
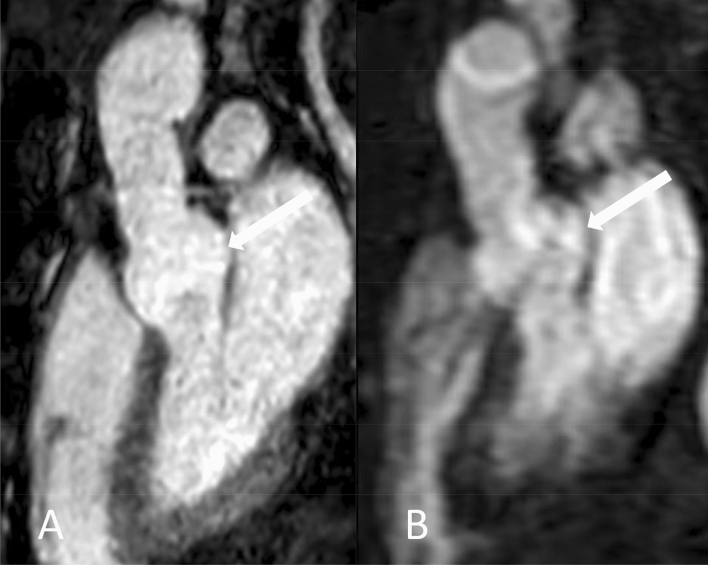
To compare a novel Compressed SENSE accelerated ECG- and respiratory-triggered flow-independent 3D isotropic Relaxation-Enhanced Angiography without Contrast and Triggering (modified REACT) with standard non-ECG-triggered 3D contrast-enhanced magnetic resonance angiography (CE-MRA) for imaging of the thoracic aorta in patients with connective tissue diseases (CTD) or other aortic diseases using manual and semiautomatic measurement approaches. This retrospective, single-center analysis of 30 patients (June-December 2018) was conducted by two radiologists, who independently measured aortic diameters on modified REACT and CE-MRA using manual (Multiplanar-Reconstruction) and semiautomatic (Advanced Vessel Analysis) measurement tools on seven levels (inner edge): Aortic annulus and sinus, sinotubular junction, mid- and high-ascending aorta, aortic isthmus, and descending aorta. Bland-Altman analysis was conducted to evaluate differences between the mean values of aortic width and ICCs were calculated to assess interobserver agreement. For each level, image quality was evaluated on a four-point scale in consensus with Wilcoxon matched-pair test used to evaluate for differences between both MRA techniques. Additionally, evaluation time for each measurement technique was noted, which was compared applying one-way ANOVA. When comparing both imaging and measurement methods, CE-MRA (mean difference 0.24 ± 0.27 mm) and the AVA-tool (- 0.21 ± 0.15 mm) yielded higher differences compared to modified REACT (- 0.11 ± 0.11 mm) and the MPR-tool (0.07 ± 0.21 mm) for all measurement levels combined without yielding clinical significance. There was an excellent interobserver agreement between modified REACT and CE-MRA using both tools of measurement (ICC > 0.9). Modified REACT (average acquisition time 06:34 ± 01:36 min) provided better image quality from aortic annulus to mid-ascending aorta (p < 0.05), whereas at distal measurement levels, no significant differences were noted. Regarding time requirement, no statistical significance was found between both measurement techniques (p = 0.08). As a novel non-CE-MRA technique, modified REACT allows for fast imaging of the thoracic aorta with higher image quality in the proximal aorta than CE-MRA enabling a reliable measurement of vessel dimensions without the need for contrast agent. Thus, it represents a clinically suitable alternative for patients requiring repetitive imaging. Manual and semiautomatic measurement approaches provided comparable results without significant difference in time need.
Keywords: Connective tissue diseases; Magnetic resonance angiography; Non-contrast-enhanced magnetic resonance angiography; Thoracic aorta.
Conflict of interest statement
The following authors of this manuscript declare relationships with the following company: Philips Healthcare. Kilian Weiss–employee; David Maintz–speakers’ bureau. Simon Lennartz–Received research support. The remaining authors declare they have no competing interests.
Figures
Similar articles
-
Imaging of the pulmonary vasculature in congenital heart disease without gadolinium contrast: Intraindividual comparison of a novel Compressed SENSE accelerated 3D modified REACT with 4D contrast-enhanced magnetic resonance angiography.J Cardiovasc Magn Reson. 2020 Jan 23;22(1):8. doi: 10.1186/s12968-019-0591-y. J Cardiovasc Magn Reson. 2020. PMID: 31969137 Free PMC article.
-
Assessment of the thoracic aorta after aortic root replacement and/or ascending aortic surgery using 3D relaxation-enhanced angiography without contrast and triggering.Front Cardiovasc Med. 2025 Mar 12;12:1532661. doi: 10.3389/fcvm.2025.1532661. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40144927 Free PMC article.
-
Three-dimensional aortic geometry mapping via registration of non-gated contrast-enhanced or gated and respiratory-navigated MR angiographies.J Cardiovasc Magn Reson. 2024 Summer;26(1):100992. doi: 10.1016/j.jocmr.2024.100992. Epub 2024 Jan 10. J Cardiovasc Magn Reson. 2024. PMID: 38211655 Free PMC article.
-
Cardiovascular magnetic resonance physics for clinicians: Part II.J Cardiovasc Magn Reson. 2012 Sep 20;14(1):66. doi: 10.1186/1532-429X-14-66. J Cardiovasc Magn Reson. 2012. PMID: 22995744 Free PMC article. Review.
-
MR Angiography for Aortic Diseases.Cardiol Clin. 2025 May;43(2):229-250. doi: 10.1016/j.ccl.2025.01.001. Cardiol Clin. 2025. PMID: 40268353 Review.
Cited by
-
Non-contrast-enhanced MR-angiography of the abdominal arteries: intraindividual comparison between relaxation-enhanced angiography without contrast and triggering (REACT) and 4D contrast-enhanced MR-angiography.Abdom Radiol (NY). 2025 Apr;50(4):1887-1898. doi: 10.1007/s00261-024-04639-4. Epub 2024 Oct 28. Abdom Radiol (NY). 2025. PMID: 39467914 Free PMC article.
-
Non-contrast free-breathing 3D cardiovascular magnetic resonance angiography using REACT (relaxation-enhanced angiography without contrast) compared to contrast-enhanced steady-state magnetic resonance angiography in complex pediatric congenital heart disease at 3T.J Cardiovasc Magn Reson. 2022 Nov 17;24(1):55. doi: 10.1186/s12968-022-00895-9. J Cardiovasc Magn Reson. 2022. PMID: 36384752 Free PMC article.
-
Review of strategies to reduce the contamination of the water environment by gadolinium-based contrast agents.Insights Imaging. 2024 Feb 27;15(1):62. doi: 10.1186/s13244-024-01626-7. Insights Imaging. 2024. PMID: 38411847 Free PMC article. Review.
-
Imaging of the extracranial internal carotid artery in acute ischemic stroke: assessment of stenosis, plaques, and image quality using relaxation-enhanced angiography without contrast and triggering (REACT).Quant Imaging Med Surg. 2022 Jul;12(7):3640-3654. doi: 10.21037/qims-21-1122. Quant Imaging Med Surg. 2022. PMID: 35782261 Free PMC article.
-
Role of Cardiovascular Magnetic Resonance to Assess Cardiovascular Inflammation.Front Cardiovasc Med. 2022 Jul 6;9:877364. doi: 10.3389/fcvm.2022.877364. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35872907 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
