

Optimal timing for surgical reconstruction of bile duct injury: meta-analysis
- PMID: 32852893
- PMCID: PMC7528508
- DOI: 10.1002/bjs5.50321
Optimal timing for surgical reconstruction of bile duct injury: meta-analysis
Abstract
Background: Major bile duct injury (BDI) after cholecystectomy generally requires surgical reconstruction by means of hepaticojejunostomy. However, there is controversy regarding the optimal timing of surgical reconstruction.
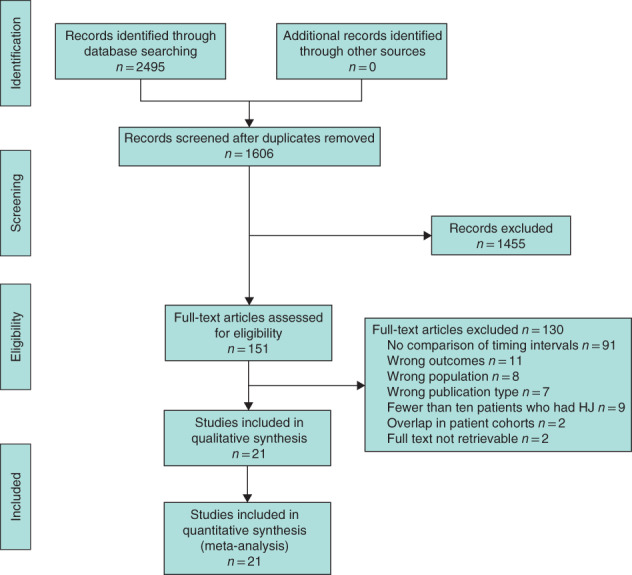
Methods: A systematic review was performed by searching PubMed, Embase and Cochrane databases for studies published between 1990 and 2018 reporting on the timing of hepaticojejunostomy for BDI (PROSPERO registration CRD42018106611). The main outcomes were postoperative morbidity, postoperative mortality and anastomotic stricture. When individual patient data were available, time intervals of these studies were attuned to render these comparable with other studies. Data for comparable time intervals were pooled using a random-effects model. In addition, data for all included studies were pooled using a generalized linear model.
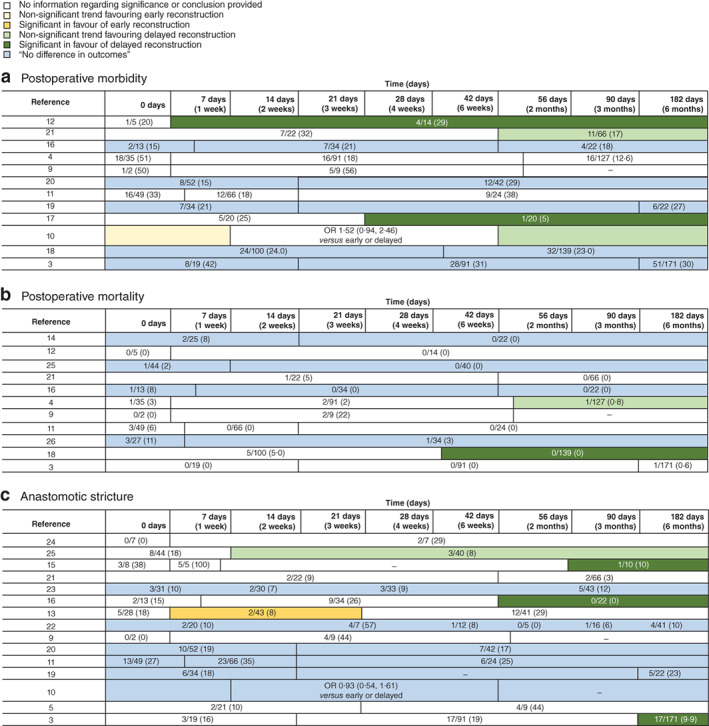
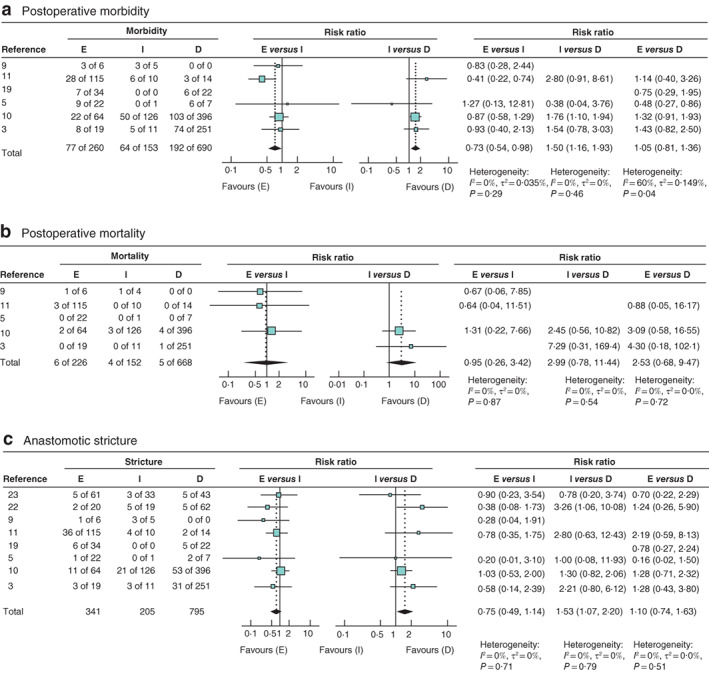
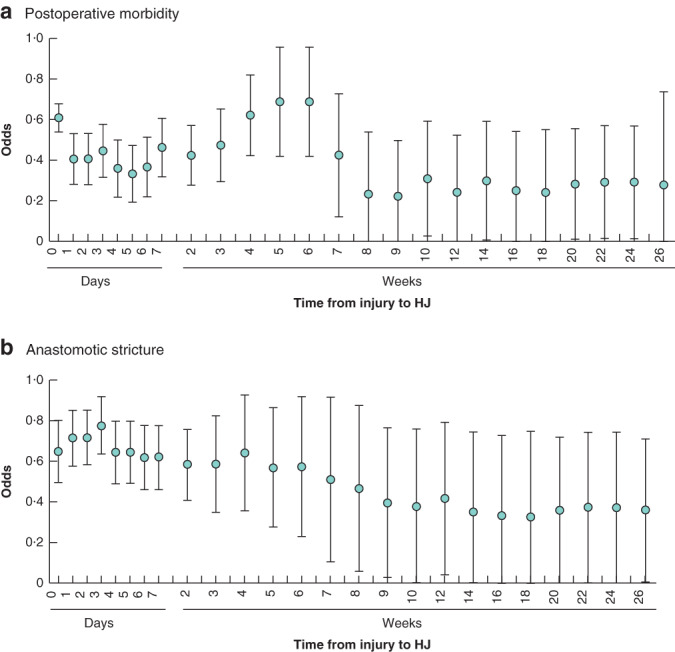
Results: Some 21 studies were included, representing 2484 patients. In these studies, 15 different time intervals were used. Eight studies used the time intervals of less than 14 days (early), 14 days to 6 weeks (intermediate) and more than 6 weeks (delayed). Meta-analysis revealed a higher risk of postoperative morbidity in the intermediate interval (early versus intermediate: risk ratio (RR) 0·73, 95 per cent c.i. 0·54 to 0·98; intermediate versus delayed: RR 1·50, 1·16 to 1·93). Stricture rate was lowest in the delayed interval group (intermediate versus delayed: RR 1·53, 1·07 to 2·20). Postoperative mortality did not differ within time intervals. The additional analysis demonstrated increased odds of postoperative morbidity for reconstruction between 2 and 6 weeks, and decreased odds of anastomotic stricture for delayed reconstruction.
Conclusion: This meta-analysis found that surgical reconstruction of BDI between 2 and 6 weeks should be avoided as this was associated with higher risk of postoperative morbidity and hepaticojejunostomy stricture.
Antecedentes: La lesión mayor de la vía biliar (bile duct injury, BDI) después de la colecistectomía generalmente requiere reconstrucción quirúrgica mediante una hepaticoyeyunostomía. Sin embargo, existe controversia en relación al momento óptimo para la reconstrucción quirúrgica. MÉTODOS: Se realizó una revisión sistemática mediante la búsqueda en las bases de datos de Pubmed, Embase y Cochrane de los estudios que proporcionaban información sobre el momento de la realización de la hepaticoyeyunostomía por la BDI, publicados entre 1990-2018 (registro PROSPERO: CRD42018106611). Los resultados principales fueron la morbilidad postoperatoria, la mortalidad postoperatoria y las estenosis de la anastomosis. Cuando se disponía de datos individuales de los pacientes, los intervalos de tiempo de estos estudios se ajustaron para hacerlos comparables con otros estudios. Los datos de los intervalos de tiempo comparables se agruparon utilizando un modelo de efectos aleatorios. Además, los datos de todos los estudios incluidos se agruparon mediante un modelo lineal generalizado.
Resultados: Se incluyeron 21 estudios con un total de 2.229 pacientes. En estos estudios, se utilizaron 15 intervalos de tiempo diferentes. Ocho estudios utilizaron los intervalos de tiempo < 14 días (precoz), 14 días-6 semanas (intermedio) y > 6 semanas (tardío). El metaanálisis reveló un mayor riesgo de morbilidad postoperatoria en el intervalo intermedio (precoz versus intermedio: riesgo relativo, RR 0,73; i.c. del 95%: 0,54-0,98; intermedio versus tardío RR 1,50, 1,16-1,93). La tasa de estenosis fue más baja en el grupo del intervalo tardío (RR intermedio versus tardío, RR 1,50, 1,07-2,20). La mortalidad postoperatoria no difirió entre los distintos intervalos de tiempo. El análisis adicional demostró mayores probabilidades de morbilidad postoperatoria para la reconstrucción entre 2-6 semanas y menores probabilidades de estenosis anastomóticas en el caso de reconstrucción tardía. CONCLUSIÓN: Este metaanálisis muestra que la reconstrucción quirúrgica de la BDI entre 2 y 6 semanas debe evitarse, ya que este intervalo se asoció con un mayor riesgo de morbilidad postoperatoria y estenosis de la hepaticoyeyunostomía.
© 2020 The Authors. BJS Open published by John Wiley & Sons Ltd on behalf of British Journal of Surgery Society.
Figures
Similar articles
-
Risk factors for anastomotic stricture after hepaticojejunostomy for bile duct injury-A systematic review and meta-analysis.Surgery. 2021 Nov;170(5):1310-1316. doi: 10.1016/j.surg.2021.05.015. Epub 2021 Jun 17. Surgery. 2021. PMID: 34148708
-
Optimal Timing of Surgical Repair After Bile Duct Injury: A Systematic Review and Meta-Analysis.Cureus. 2024 Feb 3;16(2):e53507. doi: 10.7759/cureus.53507. eCollection 2024 Feb. Cureus. 2024. PMID: 38440011 Free PMC article. Review.
-
Impact of referral pattern and timing of repair on surgical outcome after reconstruction of post-cholecystectomy bile duct injury: A multicenter study.Hepatobiliary Pancreat Dis Int. 2021 Feb;20(1):53-60. doi: 10.1016/j.hbpd.2020.10.001. Epub 2020 Oct 14. Hepatobiliary Pancreat Dis Int. 2021. PMID: 33268245
-
Surgical management of bile duct injuries sustained during laparoscopic cholecystectomy: perioperative results in 200 patients.Ann Surg. 2005 May;241(5):786-92; discussion 793-5. doi: 10.1097/01.sla.0000161029.27410.71. Ann Surg. 2005. PMID: 15849514 Free PMC article.
-
Long-term follow-up and risk factors for strictures after hepaticojejunostomy for bile duct injury: An analysis of surgical and percutaneous treatment in a tertiary center.Surgery. 2018 May;163(5):1121-1127. doi: 10.1016/j.surg.2018.01.003. Epub 2018 Feb 21. Surgery. 2018. PMID: 29475612
Cited by
-
Hepaticojejunostomy for bile duct injury: state of the art.Langenbecks Arch Surg. 2023 Feb 27;408(1):107. doi: 10.1007/s00423-023-02818-3. Langenbecks Arch Surg. 2023. PMID: 36843190 Review.
-
Waiting for bile duct dilation before repair of bile duct injury: a worthwhile strategy?Langenbecks Arch Surg. 2023 Oct 18;408(1):409. doi: 10.1007/s00423-023-03139-1. Langenbecks Arch Surg. 2023. PMID: 37848704
-
Early versus delayed reconstruction for bile duct injury a multicenter retrospective analysis of a hepatopancreaticobiliary group.Sci Rep. 2022 Jul 8;12(1):11609. doi: 10.1038/s41598-022-15978-x. Sci Rep. 2022. PMID: 35804006 Free PMC article.
-
EUS-guided biliary drainage in a patient after postcholecystectomy complete biliary transection (with video).Endosc Ultrasound. 2023 Jan-Feb;12(1):143-144. doi: 10.4103/EUS-D-21-00258. Endosc Ultrasound. 2023. PMID: 35899905 Free PMC article. No abstract available.
-
Timing of surgical repair of bile duct injuries after laparoscopic cholecystectomy: A systematic review.World J Hepatol. 2022 Feb 27;14(2):442-455. doi: 10.4254/wjh.v14.i2.442. World J Hepatol. 2022. PMID: 35317176 Free PMC article.
References
-
- Connor S, Garden OJ. Bile duct injury in the era of laparoscopic cholecystectomy. Br J Surg 2006; 93: 158–168. - PubMed
-
- Booij KAC, Coelen RJ, de Reuver PR, Besselink MG, van Delden OM, Rauws EA et al Long‐term follow‐up and risk factors for strictures after hepaticojejunostomy for bile duct injury: an analysis of surgical and percutaneous treatment in a tertiary center. Surgery 2018; 163: 1121–1127. - PubMed
-
- Rystedt J, Lindell G, Montgomery A. Bile duct injuries associated with 55 134 cholecystectomies: treatment and outcome from a national perspective. World J Surg 2016; 40: 73–80. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
