

Acute hyperkalemia in the emergency department: a summary from a Kidney Disease: Improving Global Outcomes conference
- PMID: 32852924
- PMCID: PMC7448835
- DOI: 10.1097/MEJ.0000000000000691
Acute hyperkalemia in the emergency department: a summary from a Kidney Disease: Improving Global Outcomes conference
Abstract
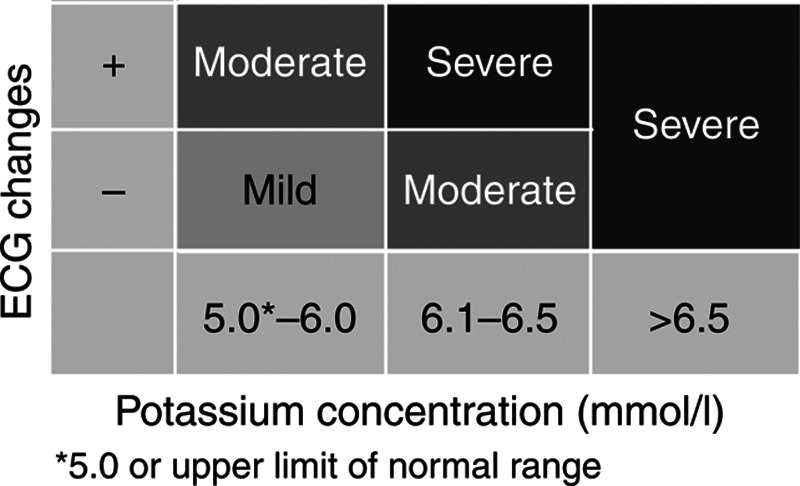
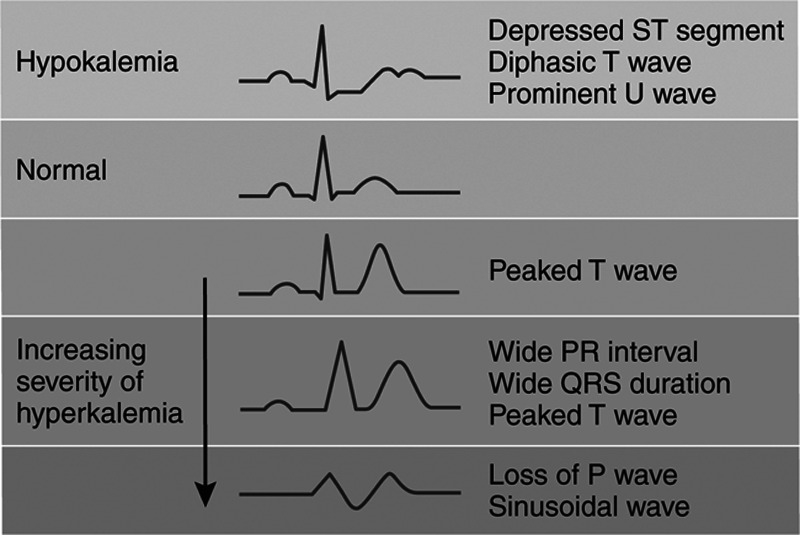
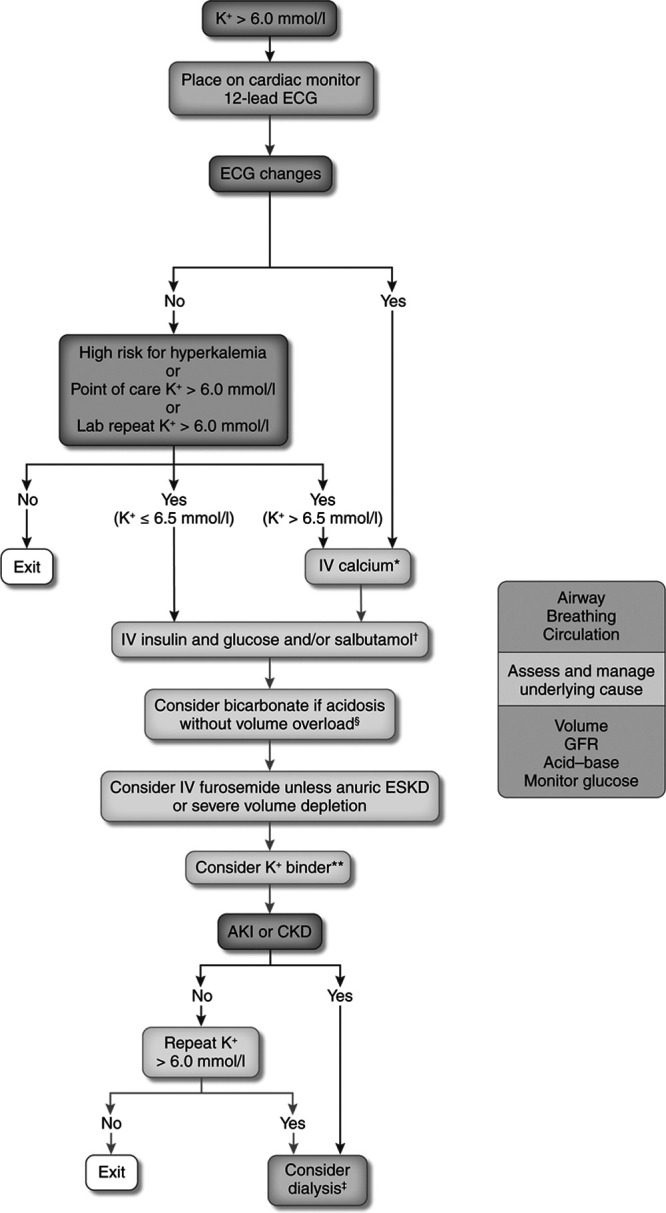
Hyperkalemia is a common electrolyte disorder observed in the emergency department. It is often associated with underlying predisposing conditions, such as moderate or severe kidney disease, heart failure, diabetes mellitus, or significant tissue trauma. Additionally, medications, such as inhibitors of the renin-angiotensin-aldosterone system, potassium-sparing diuretics, nonsteroidal anti-inflammatory drugs, succinylcholine, and digitalis, are associated with hyperkalemia. To this end, Kidney Disease: Improving Global Outcomes (KDIGO) convened a conference in 2018 to identify evidence and address controversies on potassium management in kidney disease. This review summarizes the deliberations and clinical guidance for the evaluation and management of acute hyperkalemia in this setting. The toxic effects of hyperkalemia on the cardiac conduction system are potentially lethal. The ECG is a mainstay in managing hyperkalemia. Membrane stabilization by calcium salts and potassium-shifting agents, such as insulin and salbutamol, is the cornerstone in the acute management of hyperkalemia. However, only dialysis, potassium-binding agents, and loop diuretics remove potassium from the body. Frequent reevaluation of potassium concentrations is recommended to assess treatment success and to monitor for recurrence of hyperkalemia.
Conflict of interest statement
G.L. received consultant fees and honoraria from Bayer, Fresenius Kabi, and Otsuka; travel grants from GlaxoSmithKline, Otsuka, and Pierre Fabre. C.M.C. has received consultation, advisory board membership, or research funding from Amgen, Astellas, Baxter, Boehringer Ingelheim, Janssen, Johnson & Johnson, LEO Pharma, Pfizer, and Ministry of Health Ontario; and speaker honoraria from Sanofi. C.A.H. received consultant fees from AbbVie, Amgen, AstraZeneca, Corvidia, FibroGen, Janssen, Pfizer, Relypsa, Sanifit, and University of Oxford; received research grants from Amgen, Relypsa, University of British Columbia, and Zoll; honoraria from UpToDate and is a stock-holder of Boston Scientific, Bristol-Myers Squibb, General Electric, Johnson & Johnson, and Merck. R.P.-F. received consultant fees and speaker honorarium from Akebia, AstraZeneca, Fresenius Medical Care, Novo Nordisk; speaker honoraria from AstraZeneca and Novo Nordisk; and research support from Fresenius Medical Care. Z.R. has received grants and consulting fees from Relypsa and ZS Pharma. P.R. has received consultant fees from Ablative Solutions, AstraZeneca, Bayer, Boehringer Ingelheim, Corvidia, CVRx, Fresenius, G3P, Grunenthal, Idorsia, Novartis, Novo Nordisk, Relypsa, Servier, Stealth Peptides, Vifor Fresenius Medical Care Renal Pharma. He is also a co-founder of CardioRenal. A.J.S. has received research grants and consulting fees from AstraZeneca, Bristol-Myers Squibb, Janssen, Pfizer, Portola, and Relypsa. There are no conflicts of interest for the remaining authors.
Figures
References
-
- Clase CM, Carrero JJ, Ellison DH, Grams ME, Hemmelgarn BR, Jardine MJ, et al. ; Conference Participants. Potassium homeostasis and management of dyskalemia in kidney diseases: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2020; 97:42–61 - PubMed
-
- Truhlář A, Deakin CD, Soar J, Khalifa GE, Alfonzo A, Bierens JJ, et al. ; Cardiac arrest in special circumstances section Collaborators. European resuscitation council guidelines for resuscitation 2015: section 4. Cardiac arrest in special circumstances. Resuscitation. 2015; 95:148–201 - PubMed
-
- http://www.acb.org.uk/Nat%20Lab%20Med%20Hbk/Potassium.pdf. [Accessed 12 March, 2020]
-
- Hartland AJ, Neary RH. Serum potassium is unreliable as an estimate of in vivo plasma potassium. Clin Chem. 1999; 45:1091–1092 - PubMed
-
- Cooper LB, Savarese G, Carrero JJ, Szabo B, Jernberg T, Jonsson Å, et al. Clinical and research implications of serum versus plasma potassium measurements. Eur J Heart Fail. 2019; 21:536–537 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
