

Association of Billed Advance Care Planning with End-of-Life Care Intensity for 2017 Medicare Decedents
- PMID: 32853429
- PMCID: PMC8559724
- DOI: 10.1111/jgs.16683
Association of Billed Advance Care Planning with End-of-Life Care Intensity for 2017 Medicare Decedents
Abstract
Background/objective: The Centers for Medicare & Medicaid Services (CMS) reimburses clinicians for advance care planning (ACP) discussions with Medicare patients. The objective of the study was to examine the association of CMS-billed ACP visits with end-of-life (EOL) healthcare utilization.
Design: Patient-level analyses of claims for the random 20% Medicare fee-for-service (FFS) sample of decedents in 2017. To account for multiple comparisons, Bonferroni adjusted P value <.008 was considered statistically significant.
Setting: Nationally representative sample of Medicare FFS beneficiaries.
Participants: A total of 237,989 Medicare FFS beneficiaries who died in 2017 and included those with and without a billed ACP visit during 2016-17.
Intervention: The key exposure variable was receipt of first billed ACP (none, >1 month before death).
Measurements: Six measures of EOL healthcare utilization or intensity (inpatient admission, emergency department [ED] visit, intensive care unit [ICU] stay, and expenditures within 30 days of death, in-hospital death, and first hospice within 3 days of death). Analyses was adjusted for age, race, sex, Charlson Comorbidity Index, expenditure by Dartmouth hospital referral region (high, medium, or low), and dual eligibility.
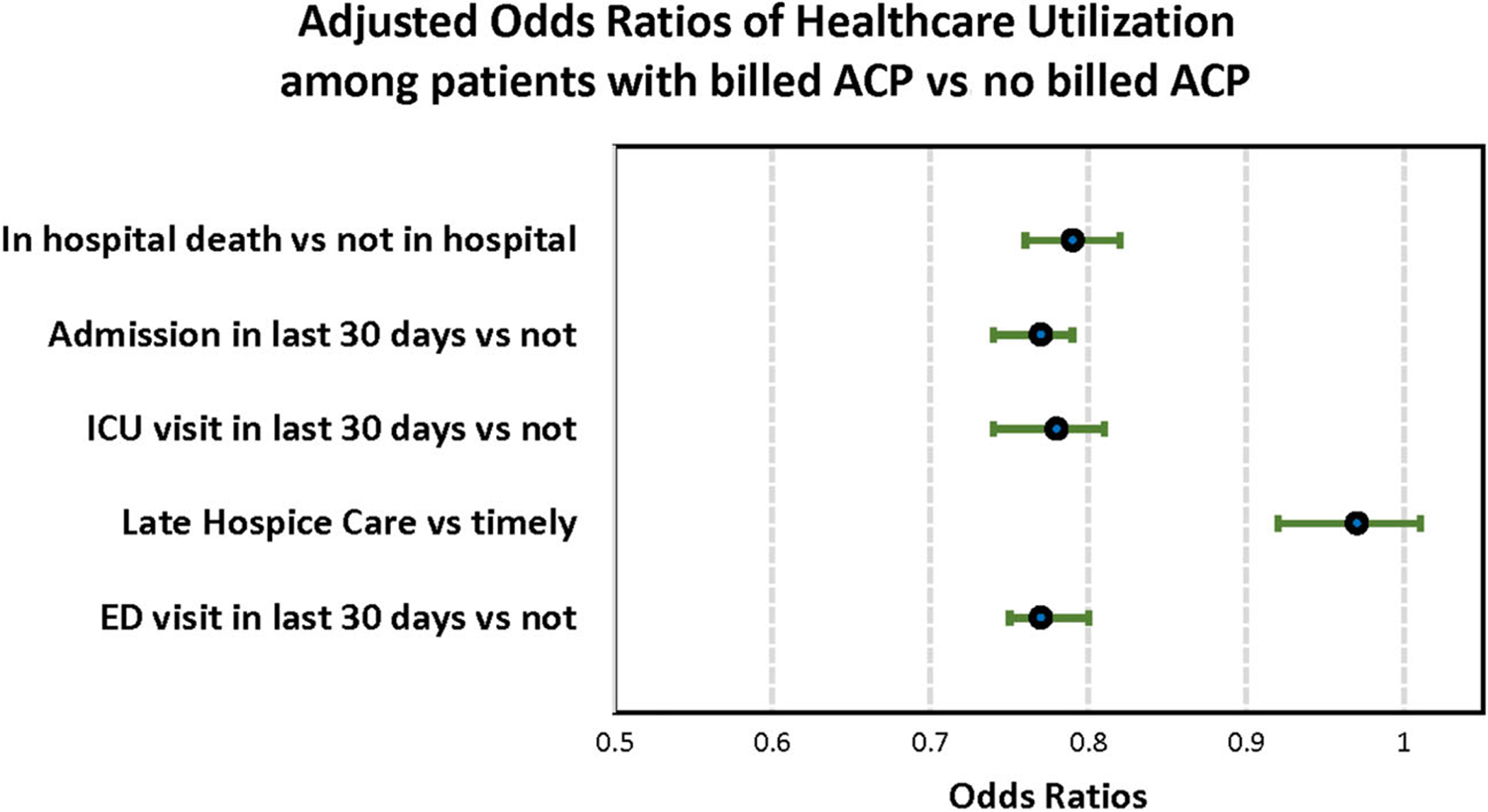
Results: Overall, 6.3% (14,986) of the sample had at least one billed ACP visit. After multivariable adjustment, patients with an ACP visit experienced significantly less intensive EOL care on four of six measures: hospitalization (odds ratio [OR] = .77; 95% confidence interval [CI] = .74-.79), ED visit (OR = .77; 95% CI = .75-.80), or ICU stay (OR = .78; 95% CI = .74-.81) within a month of death; and they were less likely to die in the hospital (OR = .79; 95% CI = .76-.82). There were no differences in the rate of late hospice enrollment (OR = .97; 95% CI = .92-1.01; P = .119) or mean expenditures ($242.50; 95% CI = -$103.63 to $588.61; P = .169).
Conclusion: Billed ACP visits were relatively uncommon among Medicare FFS decedents, but their occurrence was associated with less intensive EOL utilization. Further research on the variables affecting hospice use and expenditures in the EOL period is recommended to understand the relative role of ACP.
Keywords: Medicare; advance care planning; end of life.
© 2020 The American Geriatrics Society.
Conflict of interest statement
Figures
References
-
- OʼHanlon CE, Walling AM, Okeke E, Stevenson S, Wenger NS. A framework to guide economic analysis of advance care planning. J Palliat Med. 2018;21:1480–1485. - PubMed
-
- Gawande A. Quantity and quality of life: duties of care in life-limiting illness. JAMA. 2016;315:267–269. - PubMed
-
- Centers for Medicare & Medicaid Services. Medicare Learning Network. Advance Care Planning - Fact Sheet. Advance Care Planning https://www.cms.gov/outreach-and-education/medicare-learning-network-mln.... Accessed July 20, 2019.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
