

Cytokine release syndrome-associated encephalopathy in patients with COVID-19
- PMID: 32853434
- PMCID: PMC7461405
- DOI: 10.1111/ene.14491
Cytokine release syndrome-associated encephalopathy in patients with COVID-19
Abstract
Background and purpose: Neurological manifestations in coronavirus disease (COVID)-2019 may adversely affect clinical outcomes. Severe COVID-19 and uremia are risk factors for neurological complications. However, the lack of insight into their pathogenesis, particularly with respect to the role of the cytokine release syndrome (CRS), is currently hampering effective therapeutic interventions. The aims of this study were to describe the neurological manifestations of patients with COVID-19 and to gain pathophysiological insights with respect to CRS.
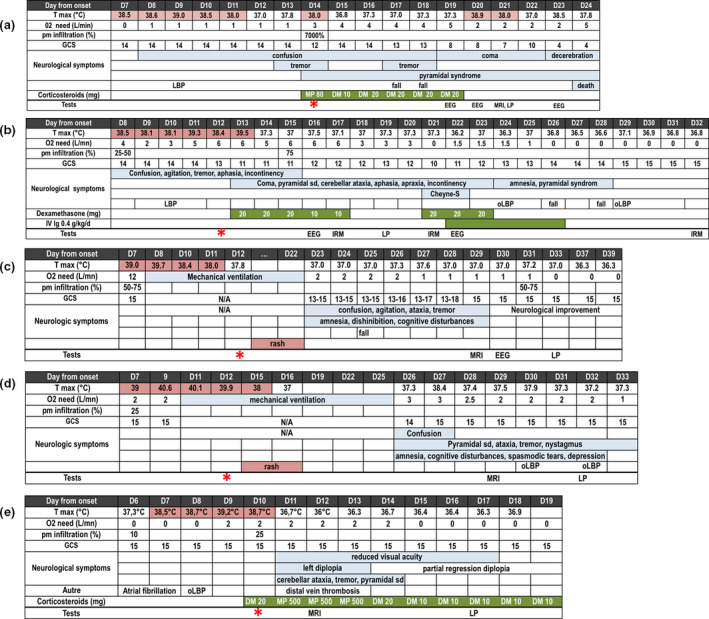
Methods: In this longitudinal study, we performed extensive clinical, laboratory and imaging phenotyping in five patients admitted to our renal unit.
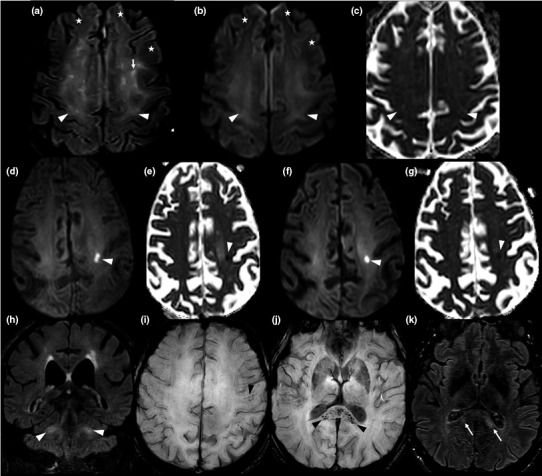
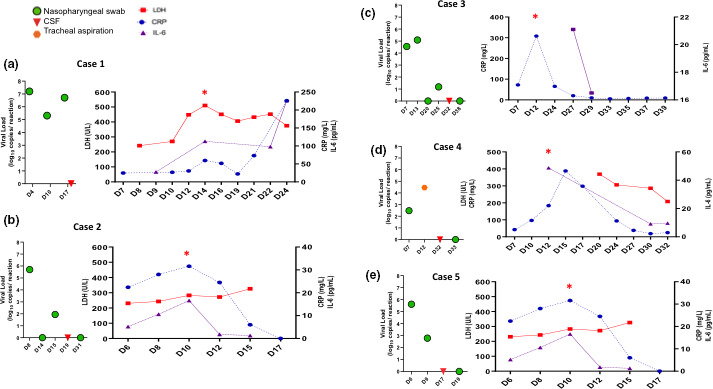
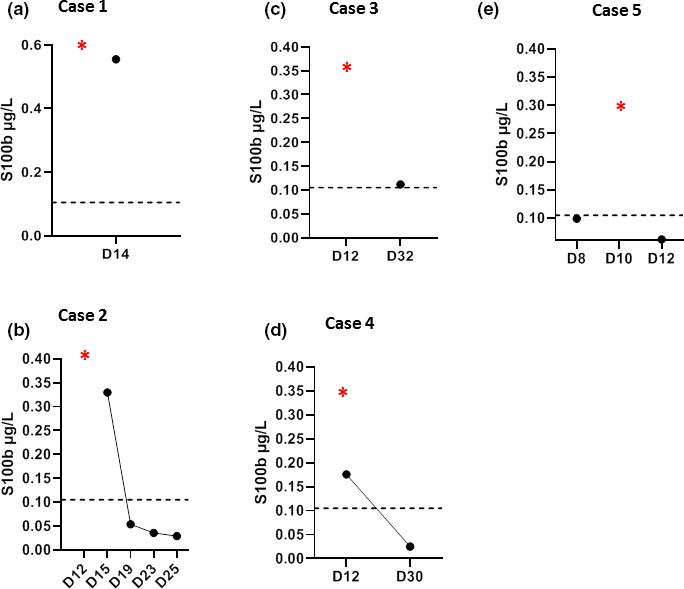
Results: Neurological presentation included confusion, tremor, cerebellar ataxia, behavioral alterations, aphasia, pyramidal syndrome, coma, cranial nerve palsy, dysautonomia, and central hypothyroidism. Notably, neurological disturbances were accompanied by laboratory evidence of CRS. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) was undetectable in the cerebrospinal fluid (CSF). Hyperalbuminorrachia and increased levels of the astroglial protein S100B were suggestive of blood-brain barrier (BBB) dysfunction. Brain magnetic resonance imaging findings comprised evidence of acute leukoencephalitis (n = 3, one of whom had a hemorrhagic form), cytotoxic edema mimicking ischaemic stroke (n = 1), or normal results (n = 2). Treatment with corticosteroids and/or intravenous immunoglobulins was attempted, resulting in rapid recovery from neurological disturbances in two cases. SARS-CoV2 was undetectable in 88 of the 90 patients with COVID-19 who underwent Reverse Transcription-PCR testing of CSF.
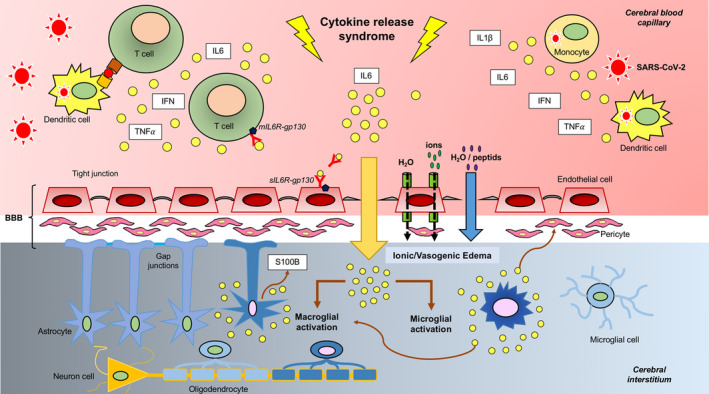
Conclusions: Patients with COVID-19 can develop neurological manifestations that share clinical, laboratory and imaging similarities with those of chimeric antigen receptor T-cell-related encephalopathy. The pathophysiological underpinnings appear to involve CRS, endothelial activation, BBB dysfunction, and immune-mediated mechanisms.
Keywords: COVID-19; corticosteroids; cytokine; encephalitis; intravenous immunoglobulins; kidney; neurological disorders.
© 2020 European Academy of Neurology.
Conflict of interest statement
The authors declare no financial or other conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
