

COVID-19 prevalence and mortality in patients with cancer and the effect of primary tumour subtype and patient demographics: a prospective cohort study
- PMID: 32853557
- PMCID: PMC7444972
- DOI: 10.1016/S1470-2045(20)30442-3
COVID-19 prevalence and mortality in patients with cancer and the effect of primary tumour subtype and patient demographics: a prospective cohort study
Erratum in
-
Correction to Lancet Oncol 2020; 21: 1309-16.Lancet Oncol. 2020 Oct;21(10):e462. doi: 10.1016/S1470-2045(20)30531-3. Epub 2020 Sep 3. Lancet Oncol. 2020. PMID: 32891190 Free PMC article. No abstract available.
Abstract
Background: Patients with cancer are purported to have poor COVID-19 outcomes. However, cancer is a heterogeneous group of diseases, encompassing a spectrum of tumour subtypes. The aim of this study was to investigate COVID-19 risk according to tumour subtype and patient demographics in patients with cancer in the UK.
Methods: We compared adult patients with cancer enrolled in the UK Coronavirus Cancer Monitoring Project (UKCCMP) cohort between March 18 and May 8, 2020, with a parallel non-COVID-19 UK cancer control population from the UK Office for National Statistics (2017 data). The primary outcome of the study was the effect of primary tumour subtype, age, and sex and on severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) prevalence and the case-fatality rate during hospital admission. We analysed the effect of tumour subtype and patient demographics (age and sex) on prevalence and mortality from COVID-19 using univariable and multivariable models.
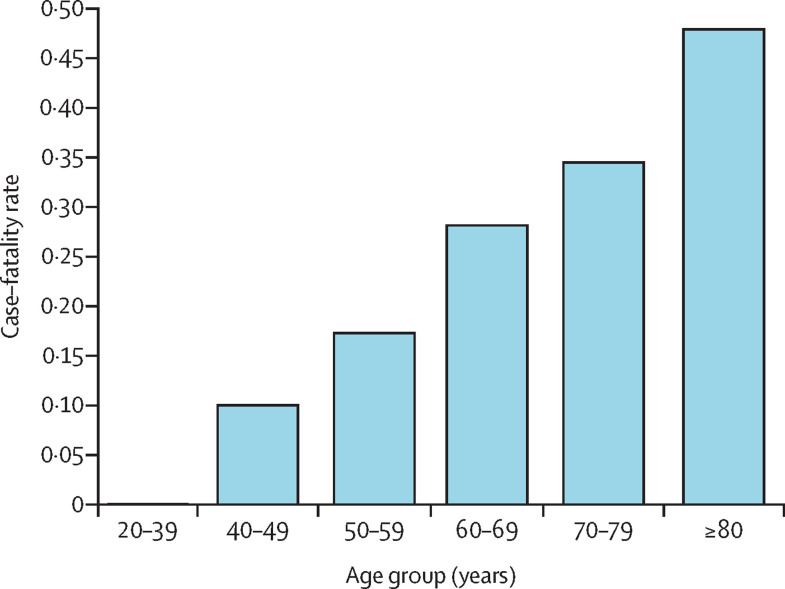
Findings: 319 (30·6%) of 1044 patients in the UKCCMP cohort died, 295 (92·5%) of whom had a cause of death recorded as due to COVID-19. The all-cause case-fatality rate in patients with cancer after SARS-CoV-2 infection was significantly associated with increasing age, rising from 0·10 in patients aged 40-49 years to 0·48 in those aged 80 years and older. Patients with haematological malignancies (leukaemia, lymphoma, and myeloma) had a more severe COVID-19 trajectory compared with patients with solid organ tumours (odds ratio [OR] 1·57, 95% CI 1·15-2·15; p<0·0043). Compared with the rest of the UKCCMP cohort, patients with leukaemia showed a significantly increased case-fatality rate (2·25, 1·13-4·57; p=0·023). After correction for age and sex, patients with haematological malignancies who had recent chemotherapy had an increased risk of death during COVID-19-associated hospital admission (OR 2·09, 95% CI 1·09-4·08; p=0·028).
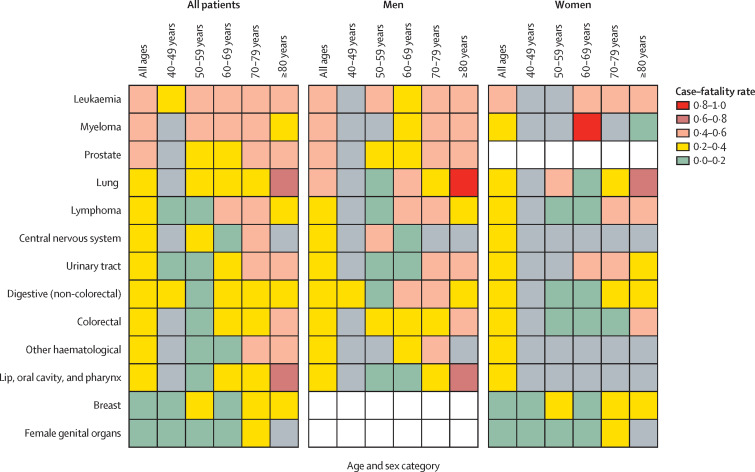
Interpretation: Patients with cancer with different tumour types have differing susceptibility to SARS-CoV-2 infection and COVID-19 phenotypes. We generated individualised risk tables for patients with cancer, considering age, sex, and tumour subtype. Our results could be useful to assist physicians in informed risk-benefit discussions to explain COVID-19 risk and enable an evidenced-based approach to national social isolation policies.
Funding: University of Birmingham and University of Oxford.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
COVID-19 in patients with cancer.Lancet Oncol. 2020 Dec;21(12):e539. doi: 10.1016/S1470-2045(20)30668-9. Lancet Oncol. 2020. PMID: 33271096 Free PMC article. No abstract available.
References
-
- WHO Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19) Feb 28, 2020. https://www.who.int/publications-detail/report-of-the-who-china-joint-mi...
-
- ESMO Cancer patient management during the COVID-19 pandemic. https://www.esmo.org/guidelines/cancer-patient-management-during-the-cov...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
