

Impact of Age on Surgical Outcomes for Locally Advanced Esophageal Cancer
- PMID: 32853569
- PMCID: PMC8023276
- DOI: 10.1016/j.athoracsur.2020.06.055
Impact of Age on Surgical Outcomes for Locally Advanced Esophageal Cancer
Abstract
Background: Older patients are often considered high-risk surgical candidates for locally advanced esophageal cancer, and the benefit of surgery in this population is unclear. This national analysis examines the effect of age on esophagectomy outcomes and compares surgery versus chemoradiation in older patients.
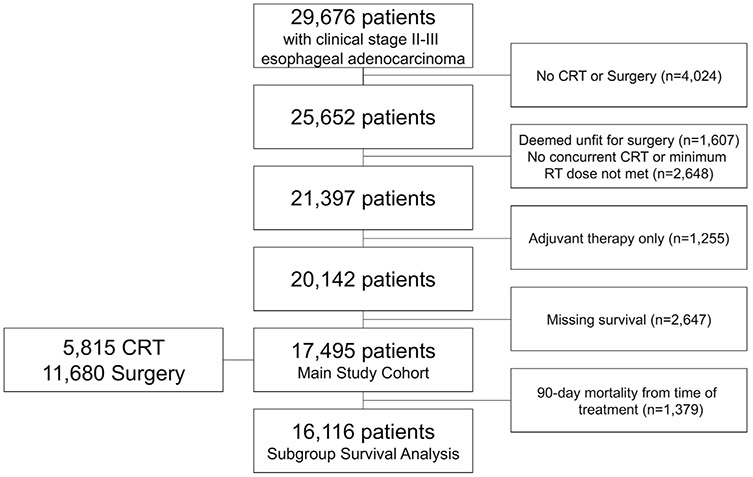
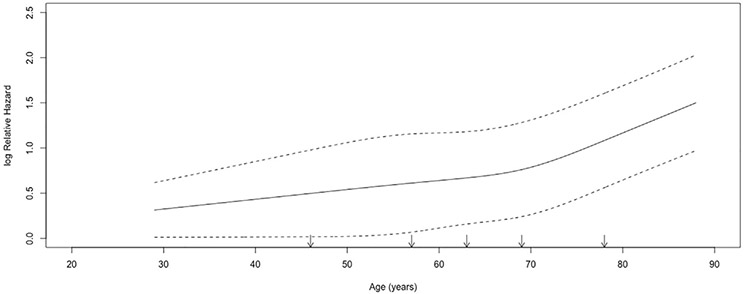
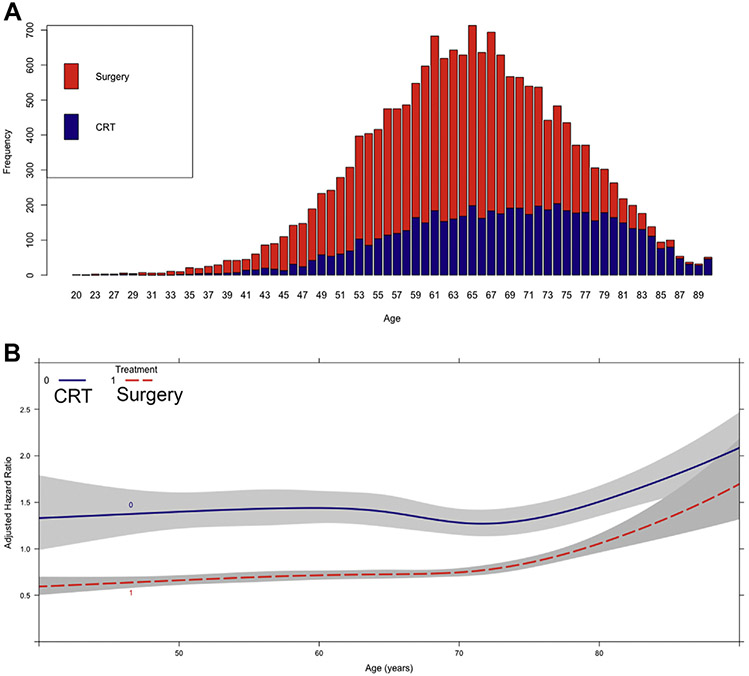
Methods: The National Cancer Database was used to identify patients with clinical stage II to III esophageal adenocarcinoma undergoing surgery or definitive chemoradiation between 2004 and 2015. Restricted cubic splines were used to examine the relationship between age and survival after esophagectomy, and maximally selected rank statistics were used to identify an age at which survival worsened. We used Cox proportional hazard models including an interaction term between age and treatment to compare overall survival, as well as survival of patients receiving esophagectomy versus definitive chemoradiation.
Results: Of 17,495 patients, 11,680 underwent esophagectomy and 5815 received chemoradiation. Survival after esophagectomy worsened with increasing age and decreased considerably after age 73 (hazard ratio = 1.05, 95% confidence interval, 1.04-1.06, per increasing year after 73 versus hazard ratio = 1.01, 95% confidence interval, 1.00-1.01, per increasing year to 73; both P < .001). Chemoradiation was increasingly used over surgery as age increased. The interaction between age and treatment was significant, and a graph of this interaction demonstrated a survival benefit for surgery over chemoradiation at most ages, including octogenarians.
Conclusions: Survival worsens with age after esophagectomy for locally advanced esophageal cancer. However, esophagectomy is associated with improved survival compared with definitive chemoradiation at most ages, including octogenarians. Esophagectomy may be considered over chemoradiation for patients who can tolerate surgery regardless of age.
Copyright © 2021 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70:7–30. - PubMed
-
- Ajani JA, D’Amico TA, Almhanna K, et al. Esophageal and esophagogastric junction cancers, version 1.2015. J Natl Compr Canc Netw. 2015;13:194–227. - PubMed
-
- van Hagen P, Hulshof MC, van Lanschot JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366:2074–2084. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
