

Admission D-dimer levels, D-dimer trends, and outcomes in COVID-19
- PMID: 32853982
- PMCID: PMC7439969
- DOI: 10.1016/j.thromres.2020.08.032
Admission D-dimer levels, D-dimer trends, and outcomes in COVID-19
Abstract
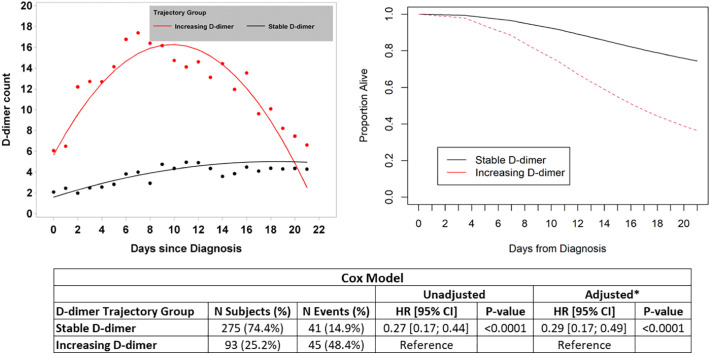
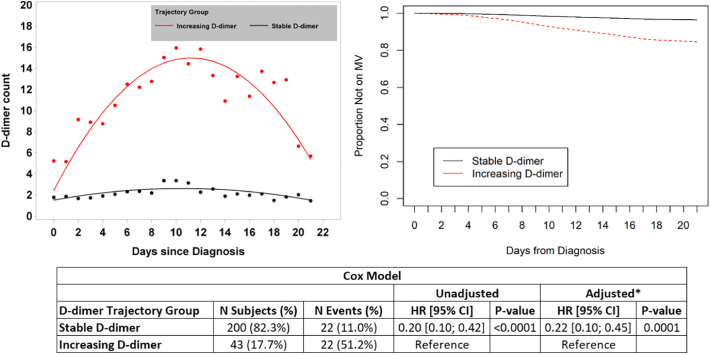
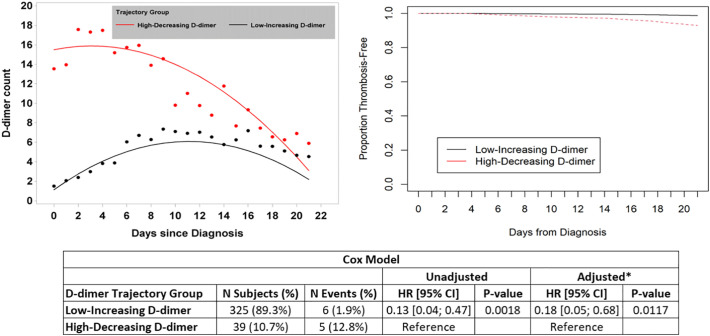
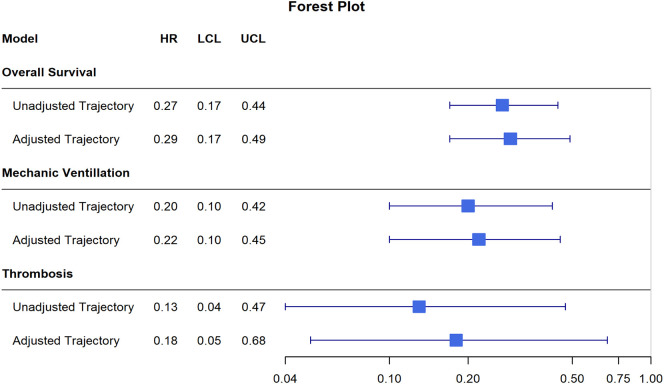
Observational data suggest an acquired prothrombotic state may contribute to the pathophysiology of COVID-19. These data include elevated D-dimers observed among many COVID-19 patients. We present a retrospective analysis of admission D-dimer, and D-dimer trends, among 1065 adult hospitalized COVID-19 patients, across 6 New York Hospitals. The primary outcome was all-cause mortality. Secondary outcomes were intubation and venous thromboembolism (VTE). Three-hundred-thirteen patients (29.4%) died, 319 (30.0%) required intubation, and 30 (2.8%) had diagnosed VTE. Using Cox proportional-hazard modeling, each 1 μg/ml increase in admission D-dimer level was associated with a hazard ratio (HR) of 1.06 (95%CI 1.04-1.08, p < 0.0001) for death, 1.08 (95%CI 1.06-1.10, p < 0.0001) for intubation, and 1.08 (95%CI 1.03-1.13, p = 0.0087) for VTE. Time-dependent receiver-operator-curves for admission D-dimer as a predictor of death, intubation, and VTE yielded areas-under-the-curve of 0.694, 0.621, and 0.565 respectively. Joint-latent-class-modeling identified distinct groups of patients with respect to D-dimer trend. Patients with stable D-dimer trajectories had HRs of 0.29 (95%CI 0.17-0.49, p < 0.0001) and 0.22 (95%CI 0.10-0.45, p = 0.0001) relative to those with increasing D-dimer trajectories, for the outcomes death and intubation respectively. Patients with low-increasing D-dimer trajectories had a multivariable HR for VTE of 0.18 (95%CI 0.05-0.68, p = 0.0117) relative to those with high-decreasing D-dimer trajectories. Time-dependent receiver-operator-curves for D-dimer trend as a predictor of death, intubation, and VTE yielded areas-under-the-curve of 0.678, 0.699, and 0.722 respectively. Although admission D-dimer levels, and D-dimer trends, are associated with outcomes in COVID-19, they have limited performance characteristics as prognostic tests.
Keywords: Admission; COVID-19; D-dimer; Outcomes; Thrombosis; Trend.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
No funding was received for the preparation of this manuscript. The authors have no relevant conflicts of interest to report.
Figures
References
-
- Wu Z., McGoogan J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020 (ahead of print) - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
