

Onodera's prognostic nutritional index correlates with tumor immune environment and survival in patients with oral squamous cell carcinoma undergoing chemoradiotherapy
- PMID: 32854035
- PMCID: PMC7452079
- DOI: 10.1016/j.tranon.2020.100850
Onodera's prognostic nutritional index correlates with tumor immune environment and survival in patients with oral squamous cell carcinoma undergoing chemoradiotherapy
Abstract
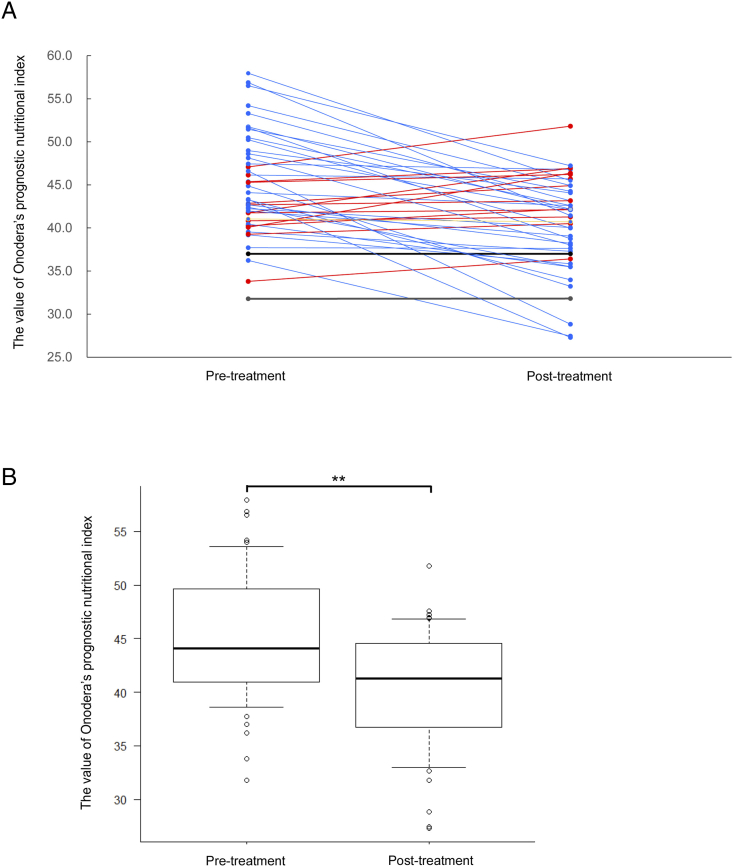
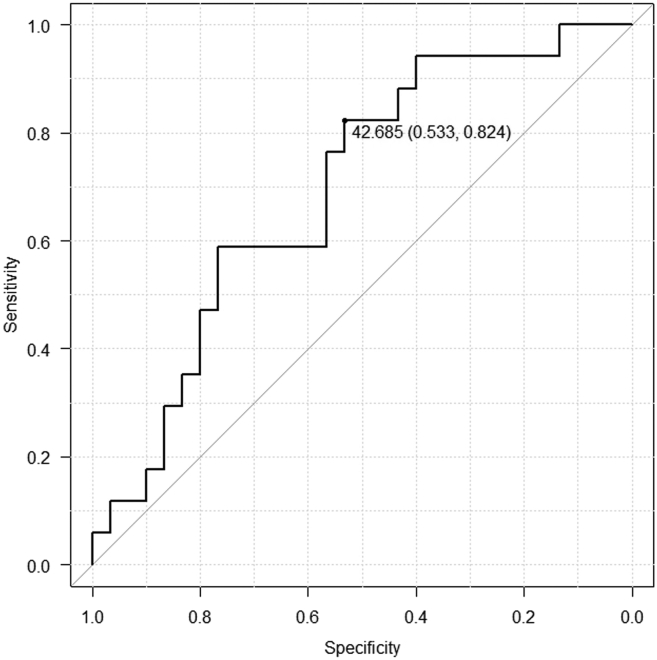
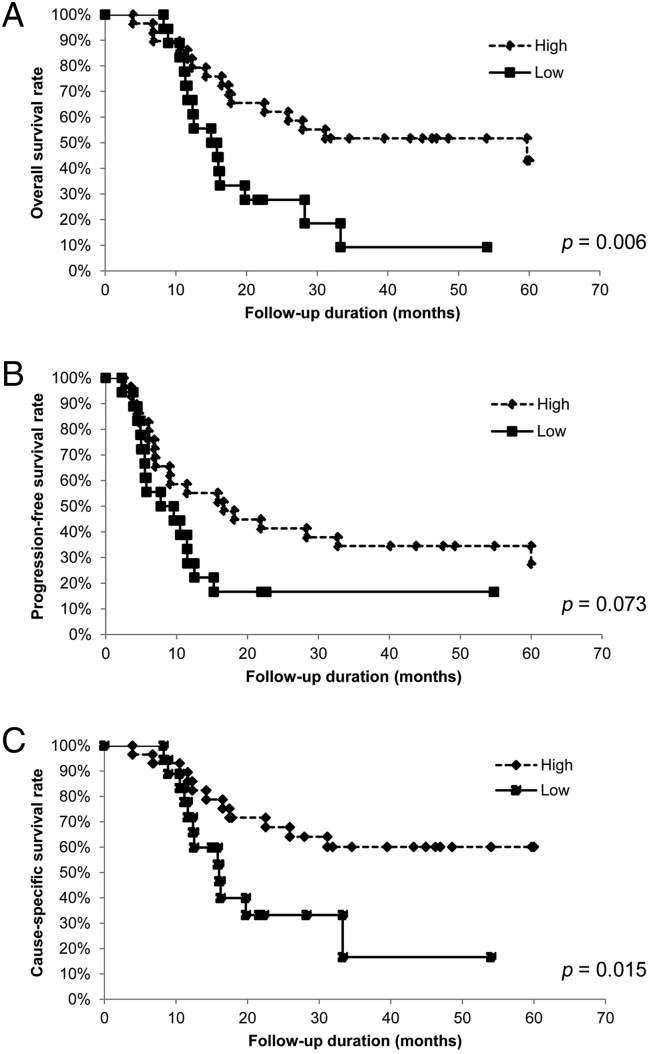
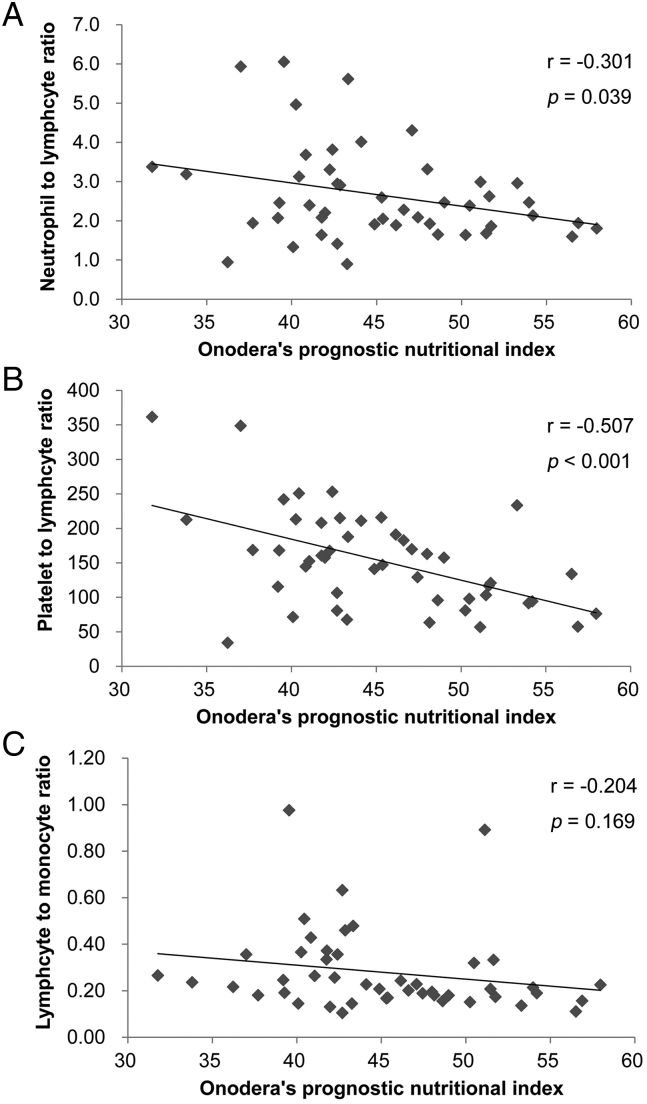
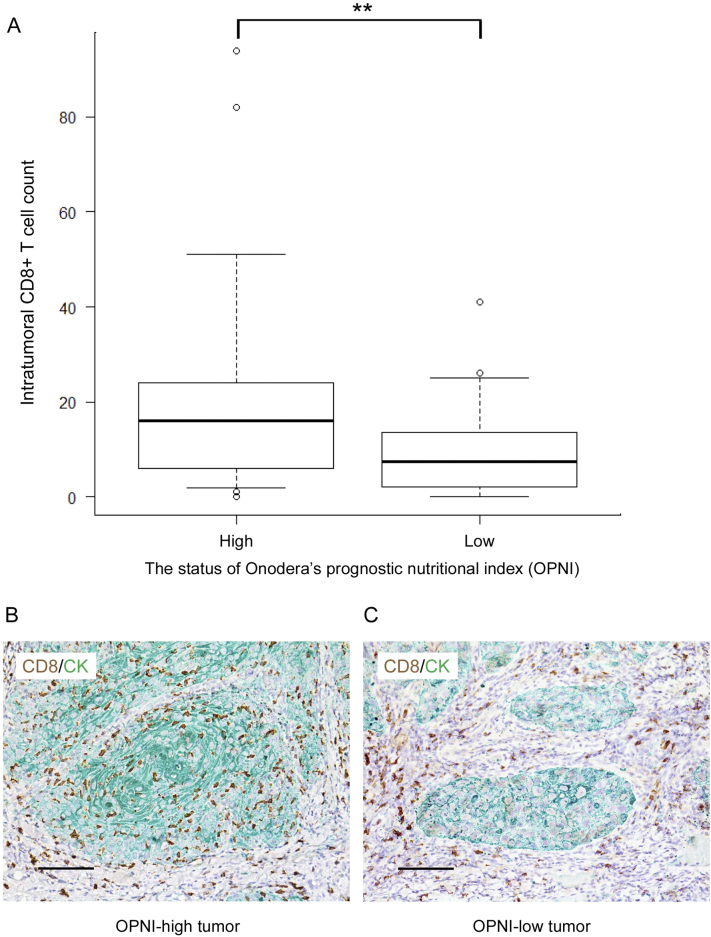
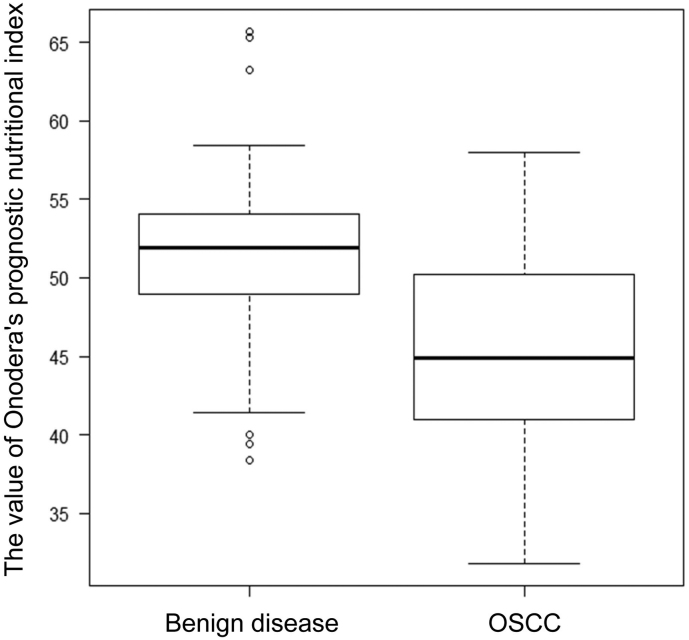
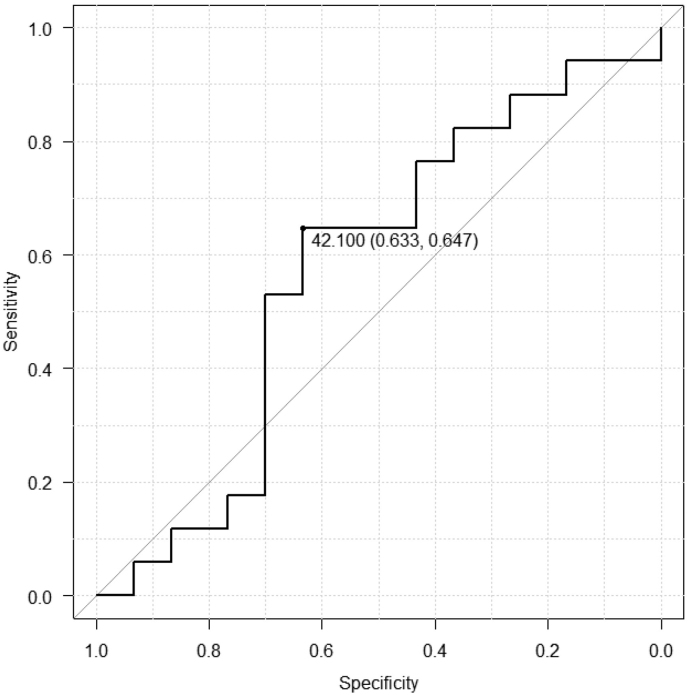
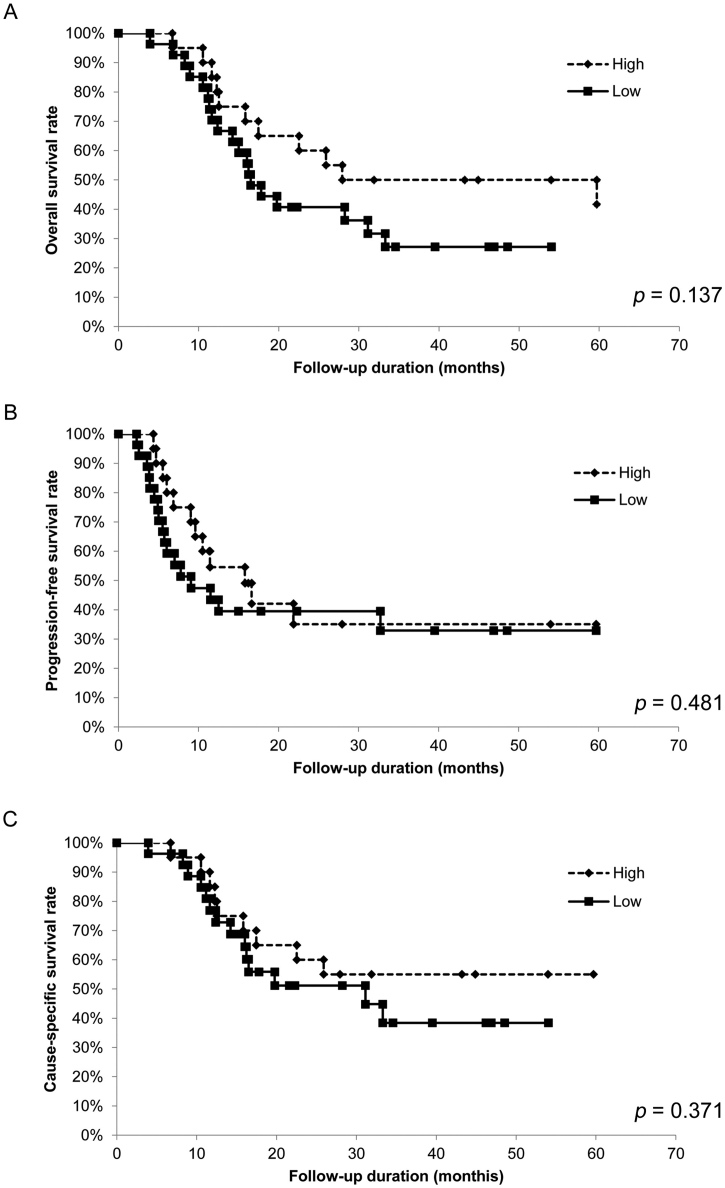
Pretreatment nutritional and immunological status is useful for predicting survival outcomes for various types of malignant tumors. Our objective was to determine the impact of the pretreatment Onodera's prognostic nutritional index (OPNI) on outcomes of patients who underwent definitive chemoradiotherapy for advanced oral squamous cell carcinoma (OSCC). We reviewed 47 patients treated for OSCC with definitive chemoradiotherapy (CRT) at our institution between January 2004 and December 2011. We determined the OPNI according to the following formula: 10 × serum albumin (g/dL) + 0.005 × total lymphocyte count (per μL). We determined the optimum OPNI cut-off through a receiver operating characteristic analysis. We analyzed the associations between OPNI status and various clinicopathological features and evaluated the effects of OPNI on the prognosis. We examined the relationships between OPNI and systemic inflammatory response parameters and analyzed intratumoral CD8+ T cells and their correlation with OPNI. The optimum OPNI cut-off was 42.7. A Kaplan-Meier curve analysis revealed that low OPNI was significantly associated with poor overall survival and cause-specific survival. The multivariate analysis revealed that low OPNI was independently correlated with poor 5 year overall survival and cause-specific survival. OPNI was significantly correlated with systemic inflammatory response parameters. Intratumoral CD8+ T cell counts in primary tumors were significantly lower for low OPNI than for high OPNI. The present data demonstrate that pretreatment OPNI is a valuable independent prognostic indicator of overall and cause-specific survival in advanced OSCC following definitive CRT. OPNI might reflect the tumor immune microenvironment characterization in OSCC.
Keywords: Chemoradiotherapy; Onodera's prognostic nutritional index; Oral squamous cell carcinoma; Tumor immune environment; prognosis.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Siegel R.L., Miller K.D., Jemal A. Cancer statistics, 2017. CA Cancer J. Clin. 2017;67(1):7–30. - PubMed
-
- Gore S.M., Crombie A.K., Batstone M.D., Clark J.R. Concurrent chemoradiotherapy compared with surgery and adjuvant radiotherapy for oral cavity squamous cell carcinoma. Head & neck. 2015;37(4):518–523. - PubMed
-
- Murakami R., Semba A., Kawahara K., Matsuyama K., Hiraki A., Nagata M. Concurrent chemoradiotherapy with S-1 in patients with stage III-IV oral squamous cell carcinoma: A retrospective analysis of nodal classification based on the neck node level. Molecular and clinical oncology. 2017;7(1):140–144. - PMC - PubMed
-
- Onodera T., Goseki N., Kosaki G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi. 1984;85(9):1001–1005. - PubMed
-
- Migita K., Takayama T., Saeki K., Matsumoto S., Wakatsuki K., Enomoto K. The prognostic nutritional index predicts long-term outcomes of gastric cancer patients independent of tumor stage. Ann. Surg. Oncol. 2013;20(8):2647–2654. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
