

Calcium channel blockers, survival and ischaemic stroke in patients with dementia: a Swedish registry study
- PMID: 32854138
- PMCID: PMC8049076
- DOI: 10.1111/joim.13170
Calcium channel blockers, survival and ischaemic stroke in patients with dementia: a Swedish registry study
Abstract
Background: The effect of calcium channel blockers (CCB) on mortality and ischaemic stroke risk in dementia patients is understudied.
Objectives: To calculate the risk of death and ischaemic stroke in dementia patients treated with CCBs, considering individual agents and dose response.
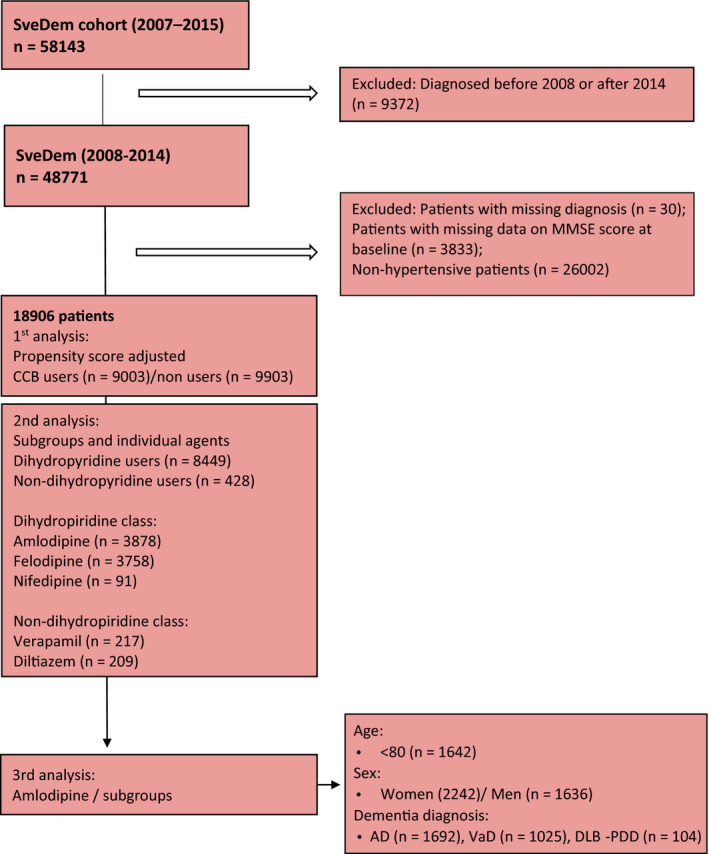
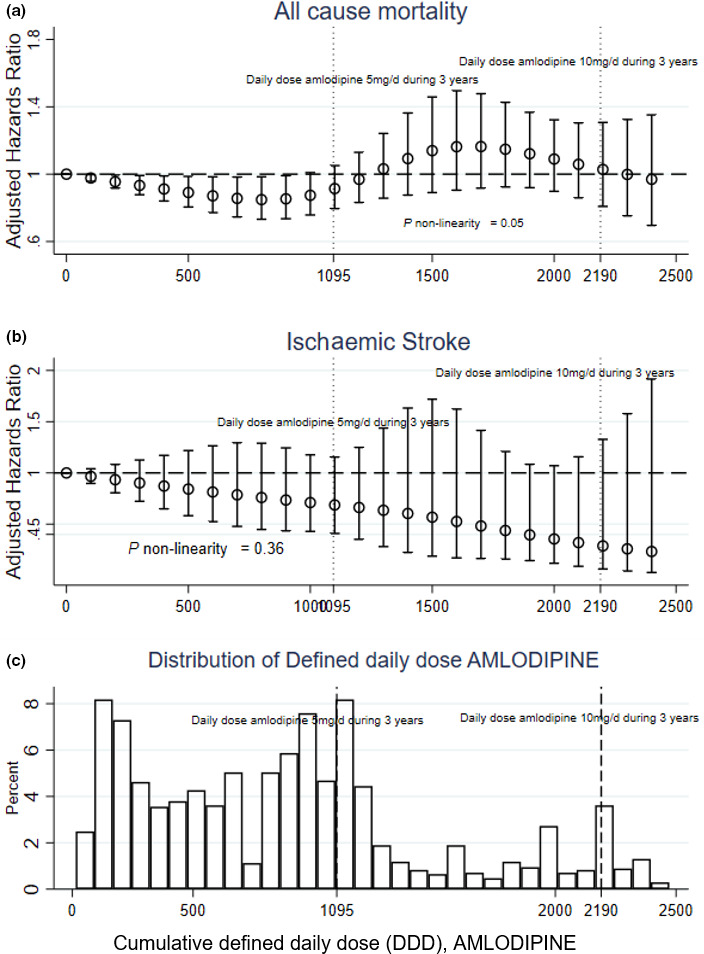
Methods: Longitudinal cohort study with 18 906 hypertensive dementia patients from the Swedish Dementia Registry (SveDem), 2008-2014. Other Swedish national registries contributed information on comorbidities, dispensed medication and outcomes. Individual CCB agents and cumulative defined daily doses (cDDD) were considered.
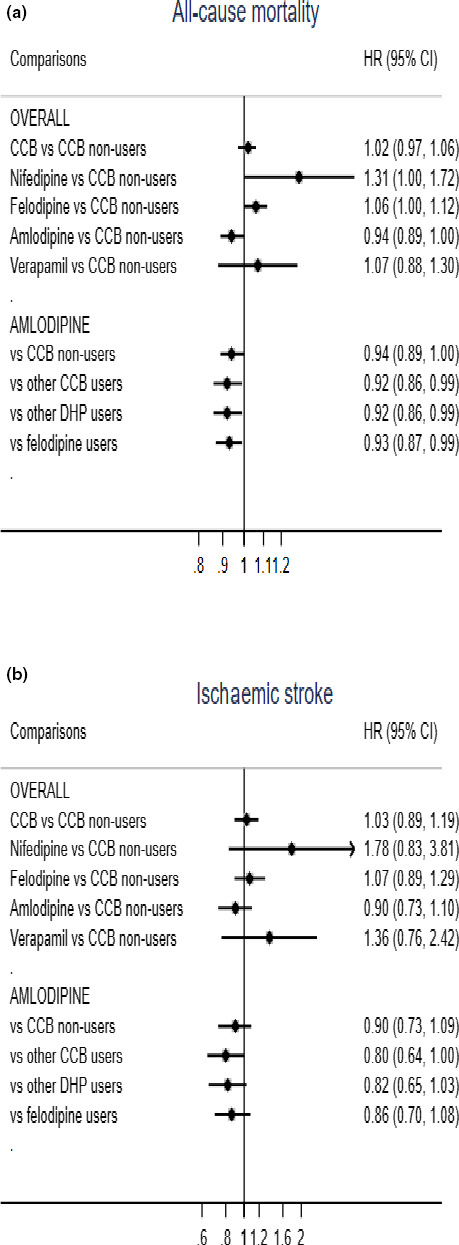
Results: In patients with hypertension and dementia, nifedipine was associated with increased mortality risk (aHR 1.32; CI 1.01-1.73; P < 0.05) compared to non-CCB users. Patients diagnosed with Alzheimer's dementia (AD) or dementia with Lewy bodies/Parkinson's disease dementia (DLB-PDD) taking amlodipine had lower mortality risk (aHR, 0.89; CI, 0.80-0.98; P < 0.05 and aHR 0.58; CI, 0.38-0.86; P < 0.01, respectively), than those taking other CCBs. Amlodipine was associated with lower stroke risk in patients with Alzheimer's dementia compared to other CCBs (aHR 0.63; CI, 0.44-0.89; P < 0.05). Sensitivity analyses with propensity score-matched cohorts repeated the results for nifedipine (aHR 1.35; 95% CI, 1.02-1.78; P < 0.05) and amlodipine in AD (aHR, 0.87; CI, 0.78-0.97; P < 0.05) and DLB-PDD (aHR, 0.56, 95%CI, 0.37-0.85; P < 0.05).
Conclusion: Amlodipine was associated with reduced mortality risk in dementia patients diagnosed with AD and DLB-PDD. AD patients using amlodipine had a lower risk of ischaemic stroke compared to other CCB users.
Keywords: alzheimer’s disease; antihypertensive drugs; calcium; dementia; mortality; stroke.
© 2020 The Authors. Journal of Internal Medicine published by John Wiley & Sons Ltd on behalf of Association for Publication of The Journal of Internal Medicine.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Garcia‐Ptacek S, Farahmand B, Kareholt I, Religa D, Cuadrado ML, Eriksdotter M. Mortality risk after dementia diagnosis by dementia type and underlying factors: a cohort of 15,209 patients based on the Swedish Dementia Registry. J Alzheimers Dis 2021; 41: 467–77. - PubMed
-
- Fitzpatrick AL, Kuller LH, Lopez OL, Kawas CH, Jagust W. Survival following dementia onset: Alzheimer's disease and vascular dementia. J Neurol Sci 2005; 230: 43–9. - PubMed
-
- Zhu L, Fratiglioni L, Guo Z, Winblad B, Viitanen M. Incidence of stroke in relation to cognitive function and dementia in the Kungsholmen Project. Neurology 2000; 54: 2103–7. - PubMed
-
- Subic A, Cermakova P, Norrving B et al. Management of acute ischaemic stroke in patients with dementia. J Intern Med 2017; 281: 348–64. - PubMed
-
- Winblad B, Amouyel P, Andrieu S et al. Defeating Alzheimer's disease and other dementias: a priority for European science and society. Lancet Neurol 2016; 15: 455–532. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
