

Treatment-Specific Associations Between Brain Activation and Symptom Reduction in OCD Following CBT: A Randomized fMRI Trial
- PMID: 32854533
- PMCID: PMC8528223
- DOI: 10.1176/appi.ajp.2020.19080886
Treatment-Specific Associations Between Brain Activation and Symptom Reduction in OCD Following CBT: A Randomized fMRI Trial
Abstract
Objective: The authors sought to examine whether brain activity is associated with treatment response to cognitive-behavioral therapy (CBT) in adolescents and adults with obsessive-compulsive disorder (OCD), and whether any associations are treatment specific relative to an active control psychotherapy (stress management therapy; SMT).
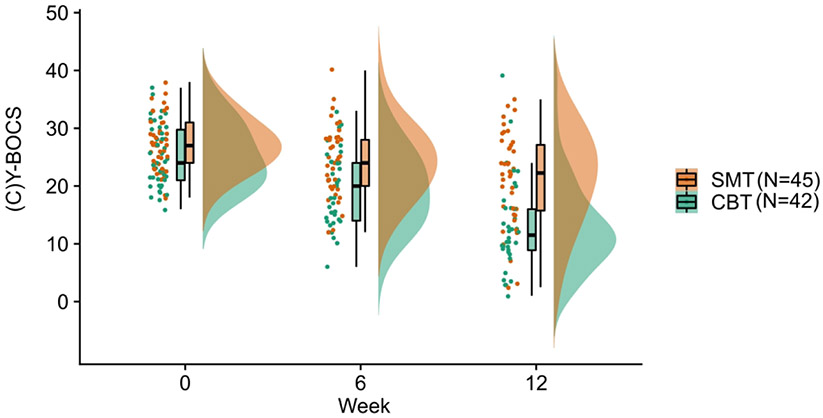
Methods: Eighty-seven patients with OCD (age range 12-45 years; 57 female, 39 medicated) were randomly assigned to receive 12 weeks of CBT or SMT. Prior to treatment, functional MRI scans were conducted in patients performing an incentive flanker task, which probes brain activation to both cognitive control and reward processing. Voxelwise linear mixed-effects models examined whether baseline brain activation was differentially associated with change in scores on the Yale-Brown Obsessive Compulsive Scale (standard or Children's version) over the course of CBT or SMT treatment.
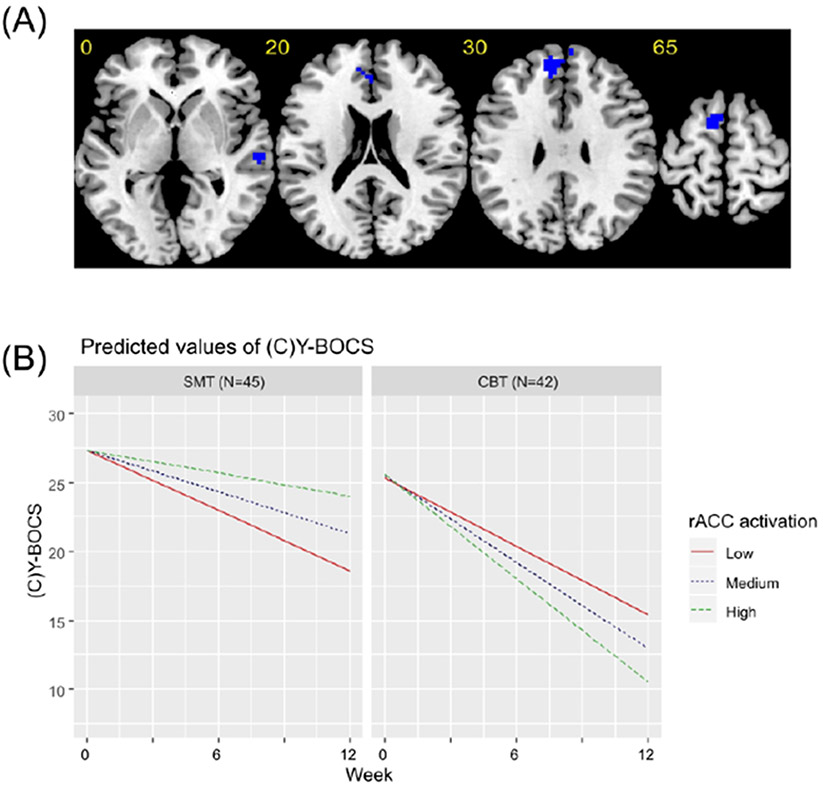
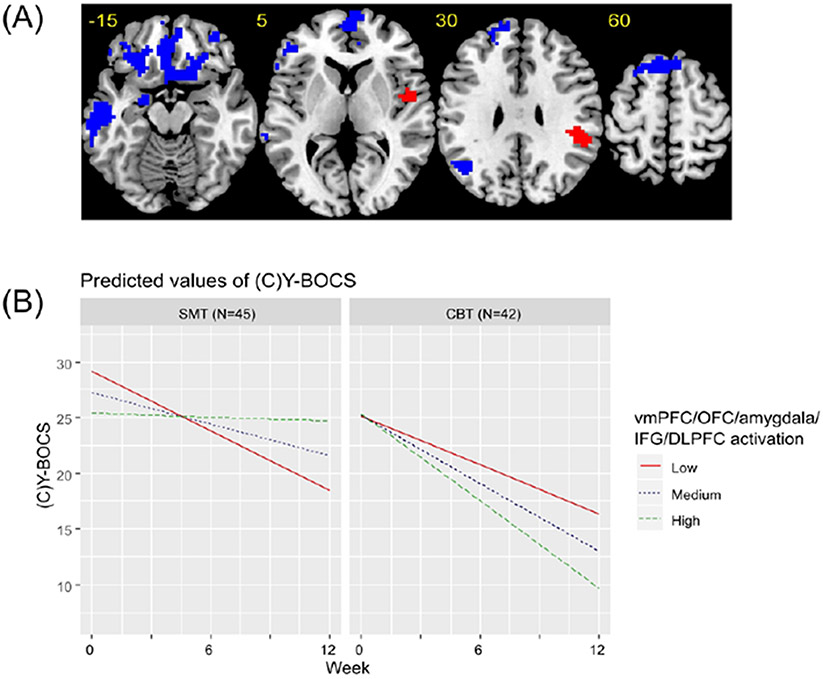
Results: Within the CBT group, a better treatment response was significantly associated with greater pretreatment activation within the right temporal lobe and rostral anterior cingulate cortex during cognitive control and within the ventromedial prefrontal, orbitofrontal, lateral prefrontal, and amygdala regions during reward processing. In contrast, reduced pretreatment activation within a largely overlapping set of regions was significantly associated with a better treatment response to SMT.
Conclusions: The study findings demonstrate that associations between brain activation and treatment response were treatment specific to CBT relative to a control psychotherapy and that these associations were stable from adolescence to mature adulthood. Such treatment-specific associations are important for the development of biomarkers to personalize treatment in OCD.
Trial registration: ClinicalTrials.gov NCT02437773.
Keywords: Cognitive-Behavioral Therapy; Inhibitory Control; Obsessive-Compulsive Disorder; Reward Processing; fMRI.
Conflict of interest statement
Conflict of Interest Disclosures
SFT has received research support from Neuronetics, St. Jude Medical (now Abbott), Boehringer–Ingelheim, and Otsuka Pharmaceutical. The remaining authors report no financial relationships with commercial interests.
Figures
References
-
- Hirschtritt ME, Bloch MH, Mathews CA: Obsessive-Compulsive Disorder: Advances in Diagnosis and Treatment. JAMA 2017; 317:1358–1367 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
