

Contemporary Management of Severe Acute Kidney Injury and Refractory Cardiorenal Syndrome: JACC Council Perspectives
- PMID: 32854844
- PMCID: PMC11032174
- DOI: 10.1016/j.jacc.2020.06.070
Contemporary Management of Severe Acute Kidney Injury and Refractory Cardiorenal Syndrome: JACC Council Perspectives
Erratum in
-
Correction.J Am Coll Cardiol. 2021 Jan 5;77(1):107-109. doi: 10.1016/j.jacc.2020.11.041. J Am Coll Cardiol. 2021. PMID: 33413934 No abstract available.
Abstract
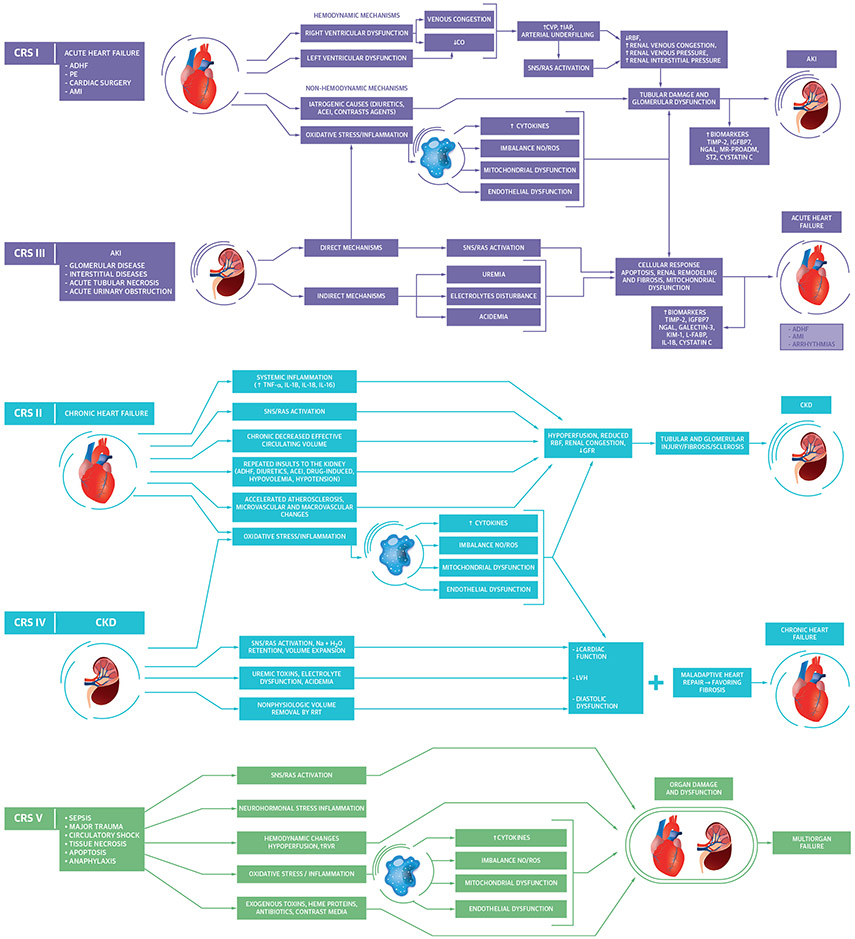
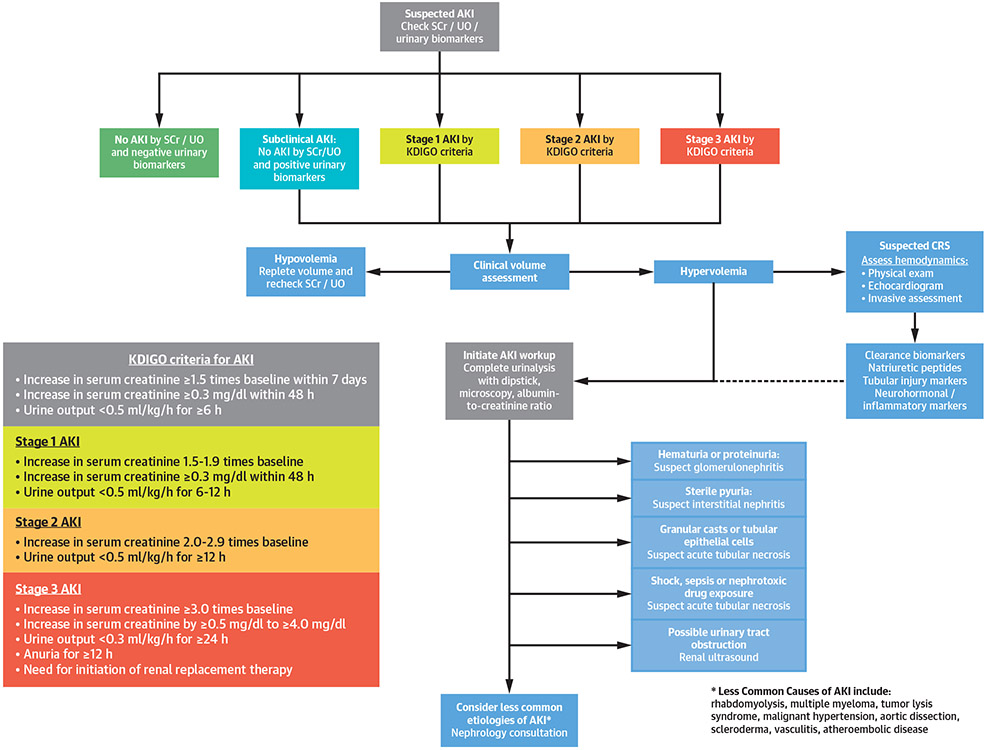
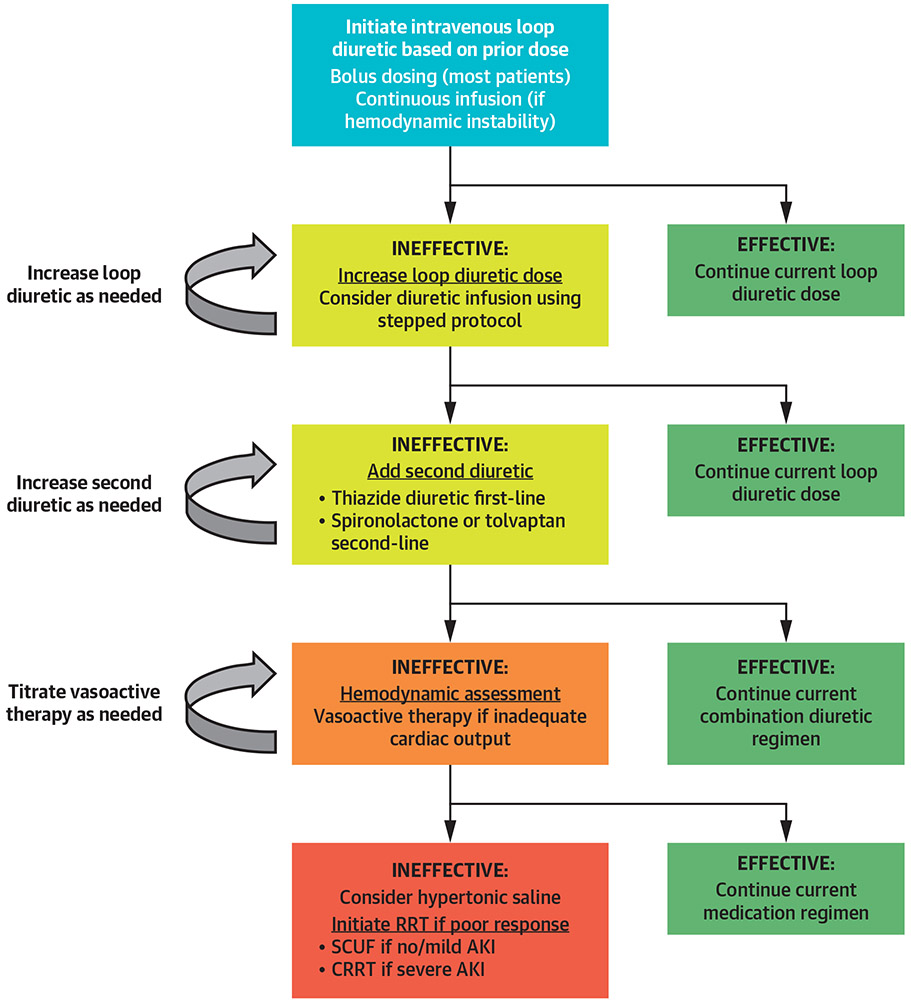
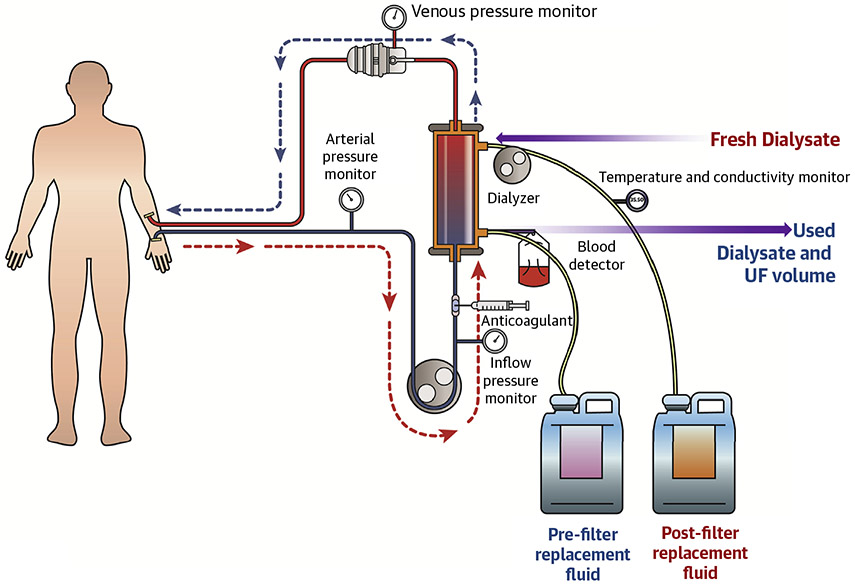
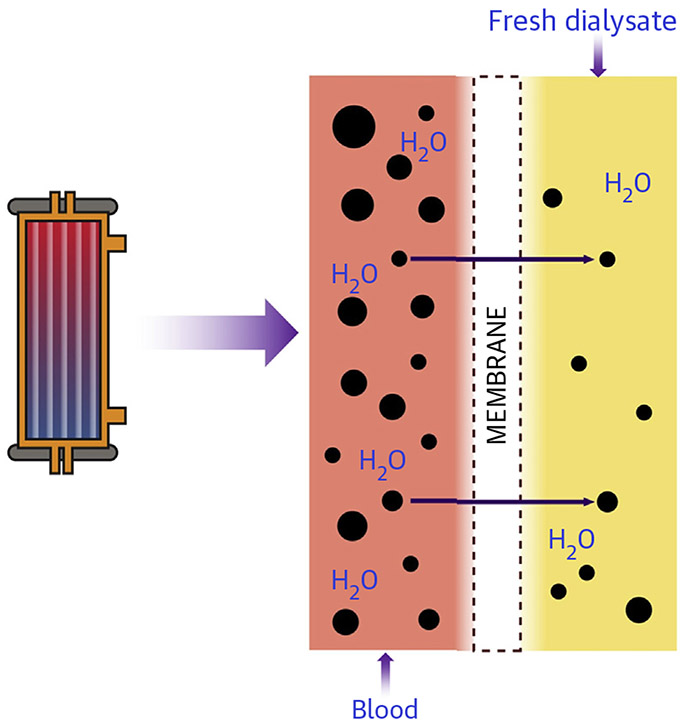
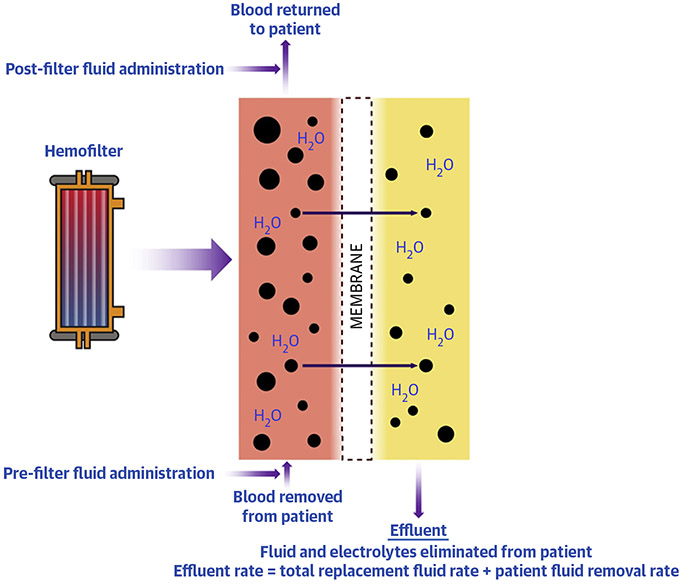
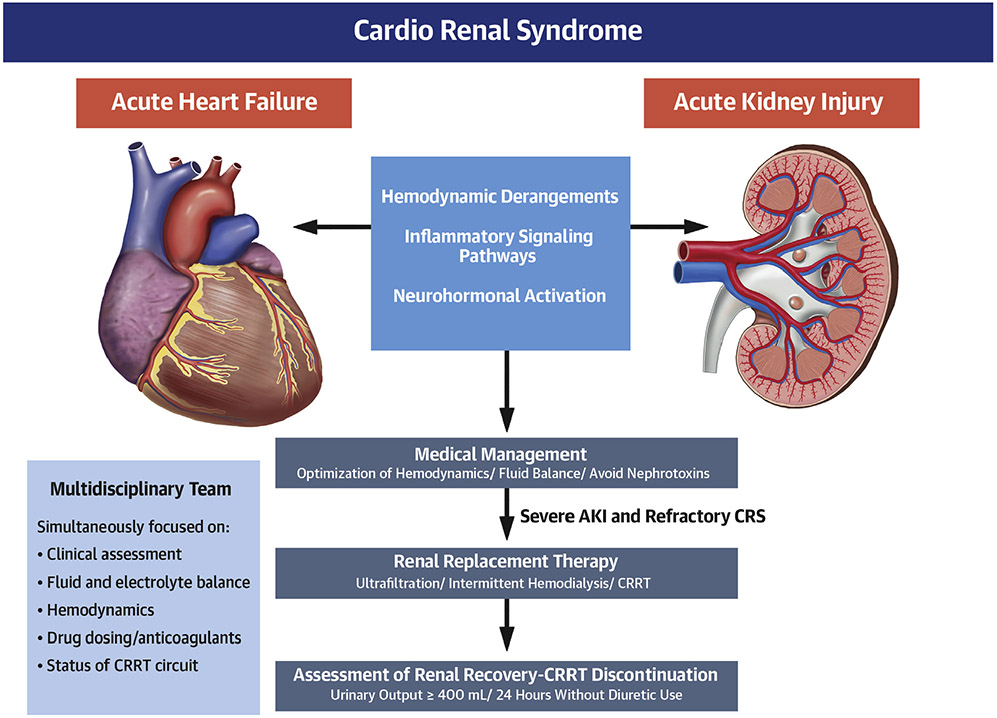
Acute kidney injury (AKI) and cardiorenal syndrome (CRS) are increasingly prevalent in hospitalized patients with cardiovascular disease and remain associated with poor short- and long-term outcomes. There are no specific therapies to reduce mortality related to either AKI or CRS, apart from supportive care and volume status management. Acute renal replacement therapies (RRTs), including ultrafiltration, intermittent hemodialysis, and continuous RRT are used to manage complications of medically refractory AKI and CRS and may restore normal electrolyte, acid-base, and fluid balance before renal recovery. Patients who require acute RRT have a significant risk of mortality and long-term dialysis dependence, emphasizing the importance of appropriate patient selection. Despite the growing use of RRT in the cardiac intensive care unit, there are few resources for the cardiovascular specialist that integrate the epidemiology, diagnostic workup, and medical management of AKI and CRS with an overview of indications, multidisciplinary team management, and transition off of RRT.
Keywords: acute kidney injury; cardiorenal syndrome; dialysis; heart failure; hemofiltration; renal replacement therapy; ultrafiltration.
Copyright © 2020 American College of Cardiology Foundation. All rights reserved.
Figures
References
-
- Jentzer JC, van Diepen S, Barsness GW, et al. Changes in comorbidities, diagnoses, therapies and outcomes in a contemporary cardiac intensive care unit population. Am Heart J 2019;215:12–9. - PubMed
-
- Jentzer JC, Chawla LS. A clinical approach to the acute cardiorenal syndrome. Crit Care Clin 2015;31:685–703. - PubMed
-
- Rangaswami J, Bhalla V, Blair JEA, et al. Cardiorenal syndrome: classification, pathophysiology, diagnosis, and treatment strategies: a scientific statement from the American Heart Association. Circulation 2019;139:e840–78. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
