

Evaluation of Nasopharyngeal Airway to Facilitate Nasotracheal Intubation
- PMID: 32855916
- PMCID: PMC7433945
- DOI: 10.4103/ams.ams_190_19
Evaluation of Nasopharyngeal Airway to Facilitate Nasotracheal Intubation
Abstract
Background and aims: Nasotracheal intubation is the most common method of airway management in oral and maxillofacial surgery patients. However, many times, it is associated with bleeding resulting from trauma to nasopharyngeal mucosa. We conducted this study to determine the effectiveness of nasopharyngeal airway (NPA) to easily facilitate the nasopharyngeal insertion and to reduce the trauma during nasotracheal intubation.
Methods: A total of 120 patients scheduled for elective oral and maxillofacial surgery requiring nasotracheal intubation were randomly divided into two groups of 60 each, after preparation with xylometazoline drops intranasally, lubrication with lignocaine jelly, and thermosoftening of the tip of the endotracheal tube (ETT). In group NPA, dilatation of the nasal cavity was done with NPA before nasotracheal intubation and in Group C, nasotracheal intubation was done without dilatation of the nasal cavity. The smoothness of insertion of ETT was graded on a 4‑point rating scale. Assessment of bleeding into nasopharynx was confirmed during laryngoscopy and was also graded with 4‑point scale.
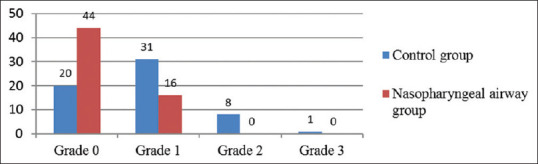
Results: In the NPA group, all the 60 (100%) patients had smooth or relatively smooth (Grade 0 or 1) insertion compared to 51 (85%) patients in the control group (P < 0.0001). Eighteen (30%) patients had mild (Grade 1) bleeding and one (1.67%) patient had moderate bleeding (Grade 2) in the control group, whereas only four (6.67%) patients in the NPA group had mild (Grade 1) bleeding (P = 0.0005).
Conclusion: Dilatation of nasal cavity with NPA significantly eases the insertion of ETT into the nasopharynx and also significantly decreases the incidence and severity of trauma and bleeding during nasotracheal intubation.
Keywords: Nasopharyngeal airway; nasotracheal intubation; oral and maxillofacial surgery.
Copyright: © 2020 Annals of Maxillofacial Surgery.
Conflict of interest statement
There are no conflicts of interest.
Figures

References
-
- Hall CE, Shutt LE. Nasotracheal intubation for head and neck surgery. Anaesthesia. 2003;58:249–56. - PubMed
-
- Elwood T, Stillions DM, Woo DW, Bradford HM, Ramamoorthy C. Nasotracheal intubation: A randomized trial of two methods. Anesthesiology. 2002;96:51–3. - PubMed
-
- O'Hanlon J, Harper KW. Epistaxis and nasotracheal intubation: Prevention with vasoconstrictor spray. Ir J Med Sci. 1994;163:58–60. - PubMed
-
- El-Seify ZA, Khattab AM, Shaaban AA, Metwalli OS, Hassan HE, Ajjoub LF. Xylometazoline pretreatment reduces nasotracheal intubation-related epistaxis in paediatric dental surgery. Br J Anaesth. 2010;105:501–5. - PubMed
-
- Kay J, Bryan R, Hart HB, Minkel DT, Munshi C. Sequential dilatation: A useful adjunct in reducing blood loss from nasotracheal intubation. Anaesthesiology. 1985;63:A259.
LinkOut - more resources
Full Text Sources