

Impact on cardiac surgery volume of a comprehensive partnership with Integrated Health Solutions
- PMID: 32856886
- PMCID: PMC7608707
- DOI: 10.1503/cjs.007519
Impact on cardiac surgery volume of a comprehensive partnership with Integrated Health Solutions
Abstract
Background: The New Brunswick Heart Centre (NBHC) entered a contractual partnership with Integrated Health Solutions (IHS) to help address increasing wait times in the province of New Brunswick.
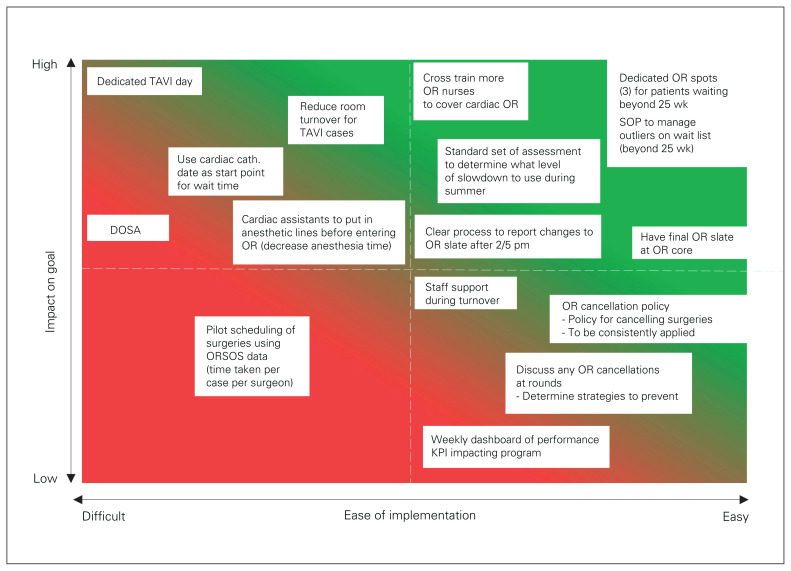
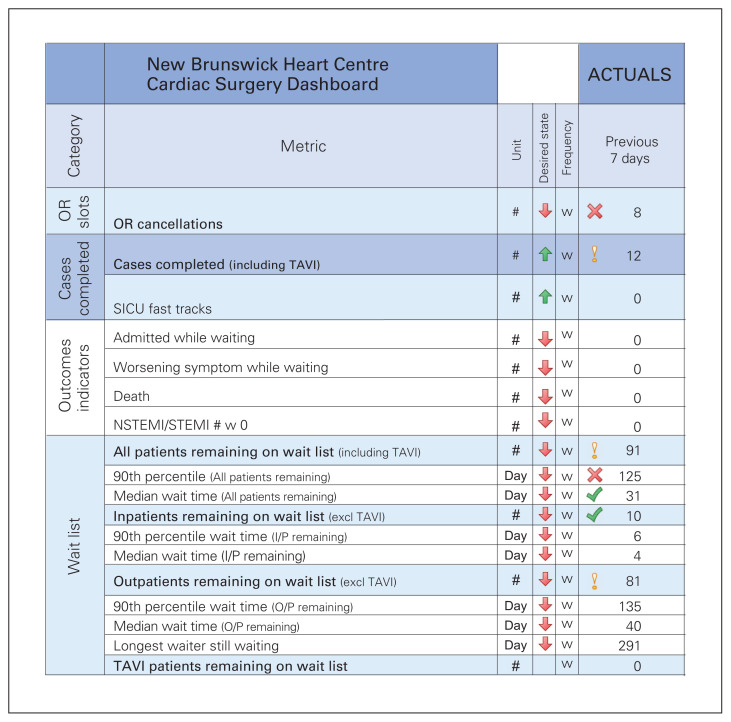
Methods: Team leaders were identified from each of the target areas, including surgeons, anesthesiologists, nurses (operating room, intensive care unit [ICU] and postoperative ward), access coordinators and administrators. The methodology used was based on Lean principles and involved exercises by stakeholders aimed at identifying opportunities for improvement. A weekly dashboard was created to monitor and facilitate improvement efforts. No additional hospital beds or operating room theatres were added during the study period.
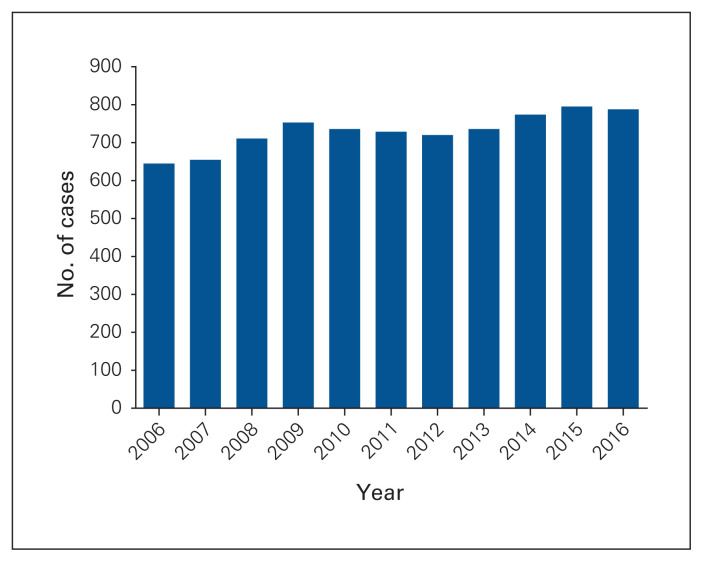
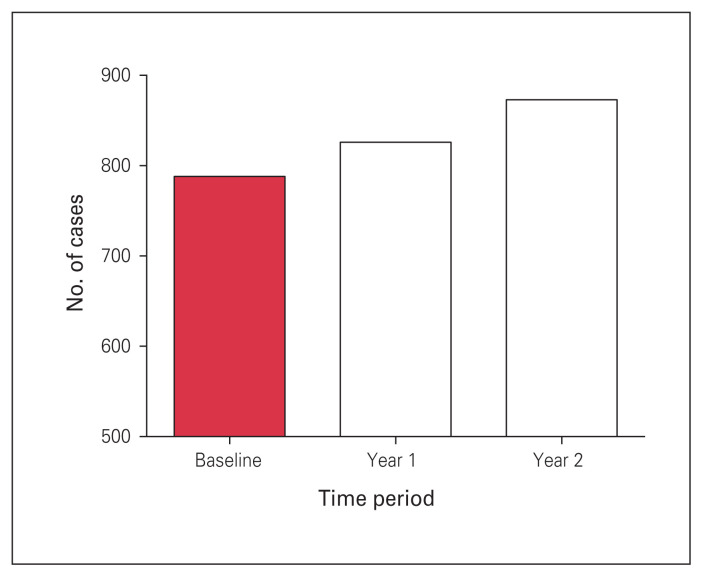
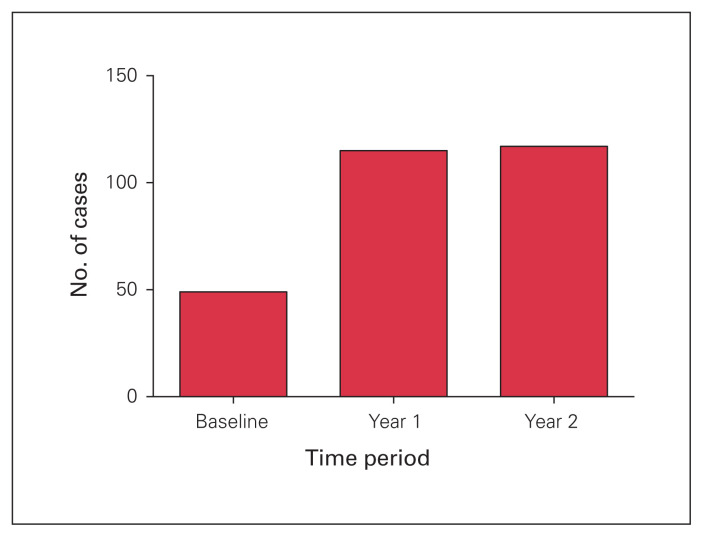
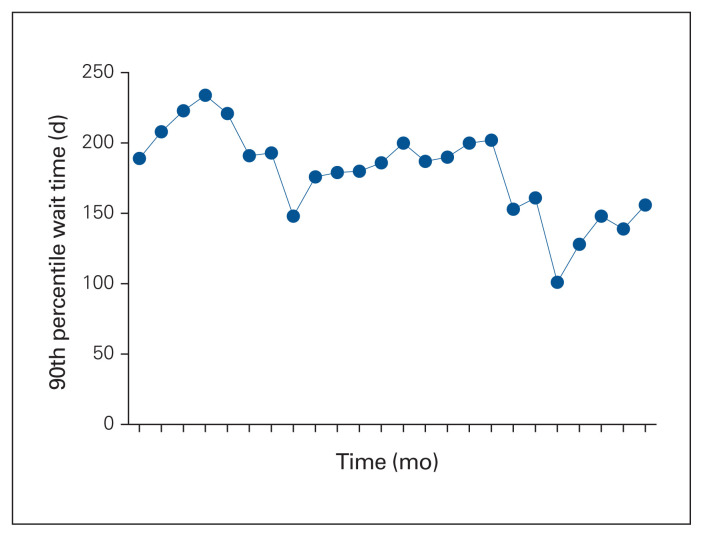
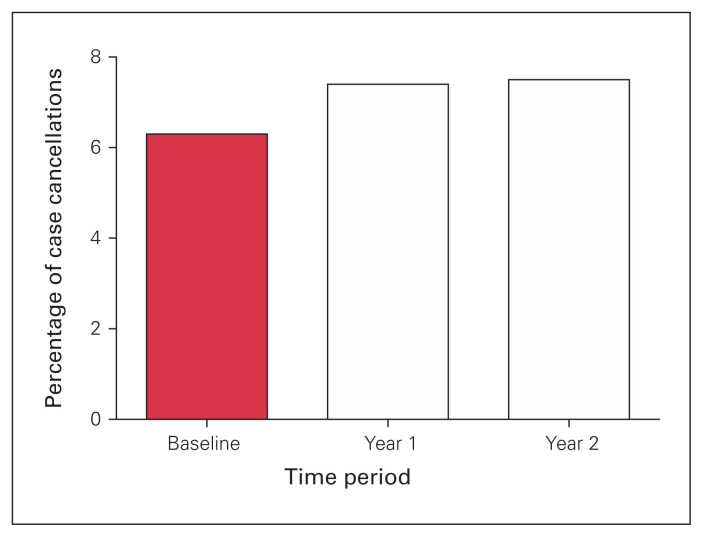
Results: After 2 years, the annual number of cardiac surgical interventions increased from 788 to 873, representing a 10.8% increase in capacity. The best median wait time for patients decreased from 52 to 35 days (35% reduction). The best 90th percentile wait time decreased from 126 to 98 days (22% reduction). The overall increase in capacity could be explained in part by the significant increase in fast tracking from the ICU to the ward (> 2-fold) or bypassing the ICU altogether (4-fold increase reaching 13%). Despite these successes, challenges persist as the number of OR cancellations remained around 7.5% of all cases, mainly because of limited ICU resources.
Conclusion: The NBHC-IHS partnership on this project has resulted in excellent engagement by stakeholders and promoted team cohesiveness. Furthermore, it has allowed significant reorganization and realignment of efforts to limit wait times and maximize overall capacity.
Contexte: Le New-Brunswick Heart Centre (NBHC) a conclu une entente contractuelle avec Integrated Health Solutions (IHS) pour remédier aux temps d’attente de plus en plus longs au Nouveau-Brunswick.
Méthodes: Des chefs d’équipe ont été identifiés pour chaque domaine cible, notamment la chirurgie, l’anesthésie, les soins infirmiers (en salle d’opération, aux soins intensifs et en soins postopératoires), la coordination des soins et la direction. La méthodologie utilisée se fondait sur l’approche Lean et comprenait des exercices visant à relever les possibilités d’amélioration. Un tableau de bord hebdomadaire a été créé pour suivre et faciliter les mesures d’amélioration. On n’a ajouté aucun lit d’hôpital et aucune salle d’opération pendant la période étudiée.
Résultats: Après 2 ans, le nombre de chirurgies cardiaques par année est passé de 788 à 873, une augmentation de 10,8 % de la capacité. Le temps d’attente médian pour les patients est tombé de 52 à 35 jours (réduction de 35 %). Le temps d’attente au 90e centile est passé de 126 à 98 jours (réduction de 22 %). L’augmentation générale de la capacité peut s’expliquer en partie par la réduction significative du temps passé aux soins intensifs avant l’admission en soins généraux (> 2 fois) ou par l’élimination complète du passage aux soins intensifs (augmentation de 400 %; 13 % des cas). Malgré ces réussites, des défis demeurent puisque le taux d’annulation des interventions est resté autour de 7,5 % des cas, surtout en raison des ressources limitées aux soins intensifs.
Conclusion: Le partenariat NBHC–IHS sur ce projet a permis de mobiliser efficacement les participants et a favorisé la cohésion au sein de l’équipe. Il a en outre permis une importante réorganisation des ressources pour réduire les temps d’attente et augmenter la capacité générale.
© 2020 Joule Inc. or its licensors.
Conflict of interest statement
This study reports the results of a partnership between the New Brunswick Heart Centre and Integrated Health Solutions (IHS), which is a service produced by Medtronic Canada. M. Zohrabi and J. Fedirko were members of the IHS team. Their primary role as authors was to ensure that the IHS process was described accurately in the article. No other competing interests were declared.
Figures
Similar articles
-
Surgical intensive care - current and future challenges?Qatar Med J. 2020 Jan 13;2019(2):3. doi: 10.5339/qmj.2019.qccc.3. eCollection 2019. Qatar Med J. 2020. PMID: 31976309 Free PMC article.
-
Effect of Lean Processes on Surgical Wait Times and Efficiency in a Tertiary Care Veterans Affairs Medical Center.JAMA Surg. 2017 Jan 1;152(1):42-47. doi: 10.1001/jamasurg.2016.2808. JAMA Surg. 2017. PMID: 27603225
-
Positive Impact of an Aortic Center Designation.Ann Vasc Surg. 2018 Jan;46:142-146. doi: 10.1016/j.avsg.2017.08.009. Epub 2017 Sep 5. Ann Vasc Surg. 2018. PMID: 28887248
-
Effectiveness of dexmedetomidine versus propofol on extubation times, length of stay and mortality rates in adult cardiac surgery patients: a systematic review and meta-analysis.JBI Database System Rev Implement Rep. 2018 May;16(5):1220-1239. doi: 10.11124/JBISRIR-2017-003488. JBI Database System Rev Implement Rep. 2018. PMID: 29762314
-
Who goes to the ICU postoperatively?Chest. 1999 May;115(5 Suppl):125S-129S. doi: 10.1378/chest.115.suppl_2.125s. Chest. 1999. PMID: 10331345 Review.
Cited by
-
Impact of management of access to cardiac surgery in the Brazilian Unified Health System at a university hospital in Campinas: pre-post analysis, 2013-2019.Epidemiol Serv Saude. 2025 Aug 4;34:e20240222. doi: 10.1590/S2237-96222025v34e20240222.en. eCollection 2025. Epidemiol Serv Saude. 2025. PMID: 40767702 Free PMC article.
-
Can Quality Improvement Methodologies Derived from Manufacturing Industry Improve Care in Cardiac Surgery? A Systematic Review.J Clin Med. 2022 Sep 12;11(18):5350. doi: 10.3390/jcm11185350. J Clin Med. 2022. PMID: 36142997 Free PMC article. Review.
References
-
- Canadian Institute for Health Information. National health expenditure trends, 1975 to 2019. Ottawa: Canadian Institute for Health Information; 2019. Available: https://www.cihi.ca/en/health-spending.
-
- Rosvall BR, Forgie K, MacLeod JB, et al. Impact of obesity on intensive care unit resource utilization after cardiac operations. Ann Thorac Surg. 2017;104:2009–15. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical