

Medication Therapy Management: 10 Years of Experience in a Large Integrated Health Care System
- PMID: 32857651
- PMCID: PMC10391185
- DOI: 10.18553/jmcp.2020.26.9.1057
Medication Therapy Management: 10 Years of Experience in a Large Integrated Health Care System
Abstract
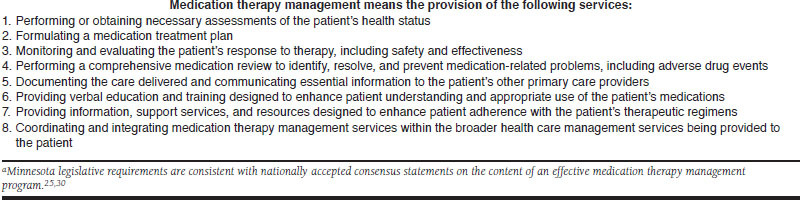
Background: Medication therapy management (MTM) was officially recognized by the federal government in the Medicare Prescription Drug, Improvement, and Modernization Act of 2003, which requires Medicare Part D plans that offer prescription drug coverage to establish MTM programs (MTMPs) for eligible beneficiaries. Even though the term "MTM" was first used in 2003, pharmacists have provided similar services since the term "pharmaceutical care" was introduced in 1990. Fairview Health Services, a large integrated health care system, implemented a standardized pharmaceutical care service system in 1998, naming it a pharmaceutical care-based MTM practice in 2006.
Objective: To present the clinical, economic, and humanistic outcomes of 10 years of delivering MTM services to patients in a health care delivery system.
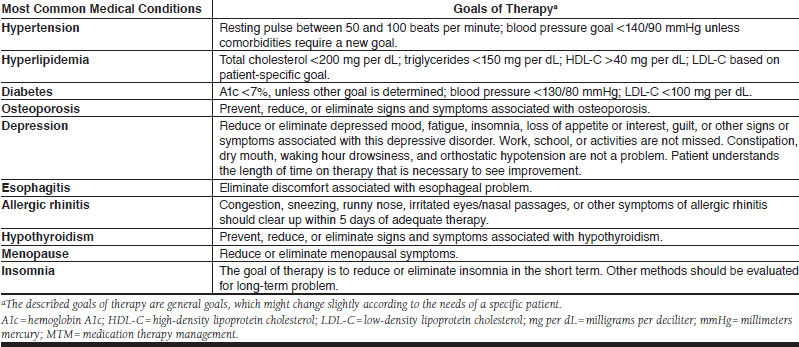
Methods: Data from MTM services provided to 9,068 patients and documented in electronic therapeutic records were retrospectively analyzed over the 10-year period from September 1998 to September 2008 in 1 health system with 48 primary care clinics. Patients eligible for MTM services were aged 21 years or older and either paid for MTM out of pocket or met their health care payer's criteria for MTM reimbursement; the criteria varied for Medicaid, Medicare, and commercially insured enrollees. All MTM was delivered face to face. Health data extracted from the electronic therapeutic record by the present study's investigators included patient demographics, medication list, medical conditions, drug therapy problems identified and addressed, change in clinical status, and pharmacist-estimated cost savings. The clinical status assessment was a comparison of the first and most recent MTM visit to measure whether the patient achieved the goals of therapy for each medical condition (e.g., the blood pressure of a patient with diabetes and hypertension will be less than 130/80 millimeters mercury [mmHg] in 1 month; the patient with allergic rhinitis will be relieved of his complaints of nasal congestion, runny nose, and eye itching within 5 days). Goals were set according to evidence-based literature and patient-specific targets determined cooperatively by pharmacists, patients, and physicians. Cost-savings calculations represented MTM pharmacists' estimates of medical services (e.g., office visits, laboratory services, urgent care visits, emergency room visits) and lost work time avoided by the intervention. All short-term (3-month) estimated health care savings that resulted from addressing drug therapy problems were analyzed. The expenses of these avoided services were calculated using the health system's contracted rates for services provided in the last quarter of 2008. The return on investment (ROI) was calculated by dividing the pharmacist-estimated savings by the cost of MTM services in 2008 (number of MTM encounters times the average cost of an MTM visit). The humanistic impact of MTM services was assessed using the results from the second patient satisfaction survey administered in 2008 (new patients seen from January through December 2008) for the health system's MTM program.
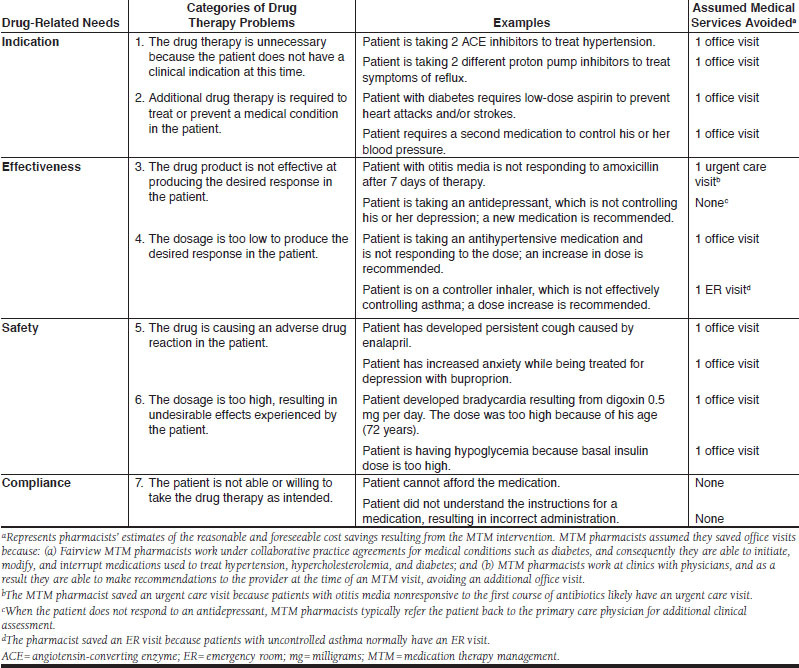
Results: A total of 9,068 patient records were in the documentation system as of September 30, 2008. During the 10-year period, there were 33,706 documented encounters (mean 3.7 encounters per patient). Of 38,631 drug therapy problems identified and addressed by MTM pharmacists, the most frequent were a need for additional drug therapy (n = 10,870, 28.1%) and subtherapeutic dosage (n = 10,100, 26.1%). In the clinical status assessment of the 12,851 medical conditions in 4,849 patients who were not at goal when they enrolled in the program, 7,068 conditions (55.0%) improved, 2,956 (23.0%) were unchanged, and 2,827 (22.0%) worsened during the course of MTM services. Pharmacist-estimated cost savings to the health system over the 10-year period were $2,913,850 ($86 per encounter) and the total cost of MTM was $2,258,302 ($67 per encounter), for an estimated ROI of $1.29 per $1 in MTM administrative costs. In the patient satisfaction survey, 95.3% of respondents agreed or strongly agreed that their overall health and well-being had improved because of MTM.
Conclusion: Pharmacist estimates of the impact of an MTM program in a large integrated health care system suggest that the program was associated with improved clinical outcomes and cost savings. Patient satisfaction with the program was high.
Disclosures: There was no external funding for this manuscript. The 3 authors are employees of Fairview Pharmacy Services. Ramalho de Oliveira had primary responsibility for the concept and design, writing, and revision of the manuscript, with the assistance of Brummel and Miller. Ramalho de Oliveira performed the data collection, and all 3 authors shared equally in data interpretation.
Conflict of interest statement
There was no external funding for this manuscript. The 3 authors are employees of Fairview Pharmacy Services. Ramalho de Oliveira had primary responsibility for the concept and design, writing, and revision of the manuscript, with the assistance of Brummel and Miller. Ramalho de Oliveira performed the data collection, and all 3 authors shared equally in data interpretation.
Figures
References
-
- Medicare Prescription Drug, Improvement, and Modernization Act of 2003, Pub. L. No. 108-173, 117 Stat. 2066 (January 7, 2003). Available at: http://www.cms.hhs.gov/MMAUpdate/downloads/hr1.pdf. Accessed March 16, 2010.
-
- Centers for Medicare and Medicaid Services. Medicare Part D medication therapy management (MTM) programs 2009 fact sheet. Updated July 21, 2009. Available at: http://www.cms.hhs.gov/PrescriptionDrugCovContra/Downloads/MTMFactSheet.pdf. Accessed March 16, 2010.
-
- Hassol A, Shoemaker SJ. Exploratory research on medication therapy management: final report. July 8, 2008. Available at: http://www.cms.hhs.gov/Reports/downloads/Blackwell.pdf. Accessed March 16, 2010.
-
- Center for Medicare and Medicaid Services. Medicare Prescription Drug Benefit Manual, Chapter 7–Medication Therapy Management and Quality Improvement Program. December 1, 2006. Available at: http://www.cms.hhs.gov/PrescriptionDrugCovContra/Downloads/PDBManual_Cha.... Accessed March 16, 2010.
-
- Cipolle RJ, Strand LM, Morley PC. Pharmaceutical Care Practice. New York: McGraw-Hill; 1998:359.
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
