

Different classes of videoscopes and direct laryngoscopes for double-lumen tube intubation in thoracic surgery: A systematic review and network meta-analysis
- PMID: 32857788
- PMCID: PMC7455027
- DOI: 10.1371/journal.pone.0238060
Different classes of videoscopes and direct laryngoscopes for double-lumen tube intubation in thoracic surgery: A systematic review and network meta-analysis
Abstract
Background: Double-lumen tube is commonly used in thoracic surgeries that need one-lung ventilation, but its big size and stiff structure make it harder to perform intubation than a conventional tracheal intubation tube.
Objectives: To investigate the effectiveness and safety of videoscopes for double-lumen tube insertion. The primary outcome was the success rate of first attempt intubation. Secondary outcomes were intubation time, malposition, oral mucosal damage, sore throat, and external manipulation.
Design: Systematic review and network meta-analysis.
Data sources: Databases (Pubmed, Embase, Cochrane, Kmbase, Web of science, Scopus) up to June 23, 2020 were searched.
Eligibility: Randomized controlled trials comparing different videoscopes for double-lumen tube intubation were included in this study.
Methods: We classified and lumped the videoscope devices into the following groups: standard (non-channeled) videolaryngoscope, channeled videolaryngoscope, videostylet, and direct laryngoscope. After assessing the quality of evidence, we statistically analyzed and chose the best device based on the surface under the cumulative ranking curve (SUCRA) by using STATA software (version 16).
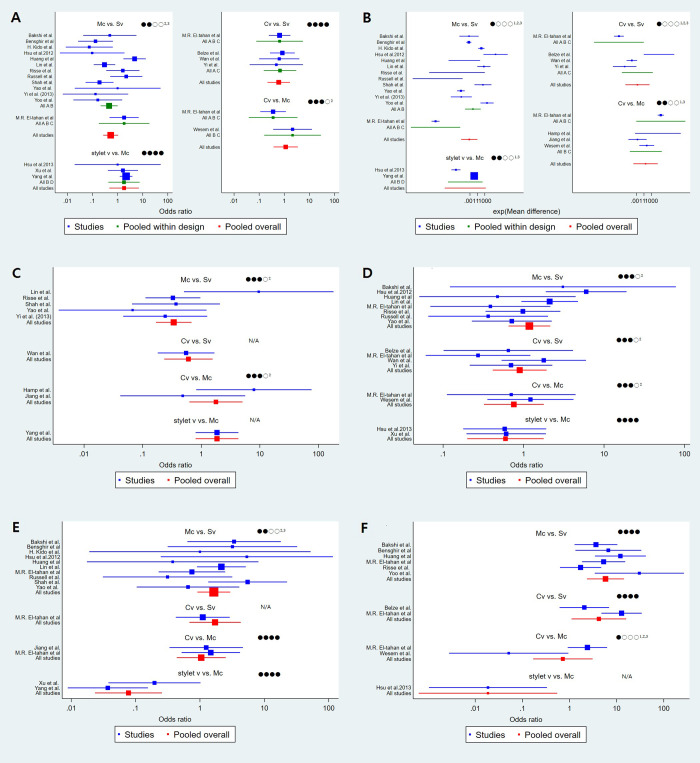
Results: We included 23 studies (2012 patients). Based on the success rate of the first attempt, a rankogram suggested that the standard videolaryngoscope (76.4 of SUCRA) was the best choice, followed by videostylet (65.5), channeled videolaryngoscope (36.1), and direct laryngoscope (22.1), respectively. However, with regard to reducing the intubation time, the best choice was videostylet, followed by a direct laryngoscope, channeled videolaryngoscope, and standard videolaryngoscope, respectively. Direct laryngoscope showed the lowest incidence of malposition but required external manipulation the most. Channeled videolaryngoscope showed the highest incidence of oral mucosal damage, but showed the lower incidence of sore throat than standard videolaryngoscope or direct laryngoscope.
Conclusion: Most videoscopes improved the success rate of double-lumen tube intubation; however, they were time-consuming (except videostylet) and had a higher malposition rate than the direct laryngoscope.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures





Similar articles
-
Comparison of the GlideScope® videolaryngoscope and the Macintosh laryngoscope for double-lumen tube intubation.Anaesthesia. 2012 Apr;67(4):411-5. doi: 10.1111/j.1365-2044.2011.07049.x. Epub 2012 Feb 11. Anaesthesia. 2012. PMID: 22324297 Clinical Trial.
-
A comparison of the McGrath® Series 5 videolaryngoscope and Macintosh laryngoscope for double-lumen tracheal tube placement in patients with a good glottic view at direct laryngoscopy.Anaesthesia. 2015 Jul;70(7):810-7. doi: 10.1111/anae.13040. Epub 2015 Feb 27. Anaesthesia. 2015. PMID: 25721326
-
GlideScope® versus C-MAC®(D) videolaryngoscope versus Macintosh laryngoscope for double lumen endotracheal intubation in patients with predicted normal airways: a randomized, controlled, prospective trial.BMC Anesthesiol. 2020 May 20;20(1):119. doi: 10.1186/s12871-020-01012-y. BMC Anesthesiol. 2020. PMID: 32434470 Free PMC article. Clinical Trial.
-
Videolaryngoscopy vs. Macintosh laryngoscopy for double-lumen tube intubation in thoracic surgery: a systematic review and meta-analysis.Anaesthesia. 2018 Aug;73(8):997-1007. doi: 10.1111/anae.14226. Epub 2018 Feb 6. Anaesthesia. 2018. PMID: 29405258
-
Airway devices for awake tracheal intubation in adults: a systematic review and network meta-analysis.Br J Anaesth. 2021 Oct;127(4):636-647. doi: 10.1016/j.bja.2021.05.025. Epub 2021 Jul 22. Br J Anaesth. 2021. PMID: 34303493
Cited by
-
Role of Lung Ultrasound in Confirmation of Double Lumen Endotracheal Tube Placement for Thoracic Surgeries: A Prospective Diagnostic Accuracy Study.Anesth Pain Med. 2022 Nov 21;12(5):e132312. doi: 10.5812/aapm-132312. eCollection 2022 Oct. Anesth Pain Med. 2022. PMID: 36937173 Free PMC article.
-
Comparisons of Videolaryngoscopes for Intubation Undergoing General Anesthesia: Systematic Review and Network Meta-Analysis of Randomized Controlled Trials.J Pers Med. 2022 Feb 26;12(3):363. doi: 10.3390/jpm12030363. J Pers Med. 2022. PMID: 35330362 Free PMC article. Review.
-
Recent Advances in Videolaryngoscopy for One-Lung Ventilation in Thoracic Anesthesia: A Narrative Review.Front Med (Lausanne). 2022 Jun 13;9:822646. doi: 10.3389/fmed.2022.822646. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35770016 Free PMC article. Review.
-
Efficacy and Safety of Video-Laryngoscopy versus Direct Laryngoscopy for Double-Lumen Endotracheal Intubation: A Systematic Review and Meta-Analysis.J Clin Med. 2021 Nov 25;10(23):5524. doi: 10.3390/jcm10235524. J Clin Med. 2021. PMID: 34884226 Free PMC article.
-
Comparison of direct and indirect images and hemodynamic response of two different video laryngoscopes to tracheal intubation.BMC Anesthesiol. 2025 Feb 20;25(1):86. doi: 10.1186/s12871-025-02966-7. BMC Anesthesiol. 2025. PMID: 39979796 Free PMC article. Clinical Trial.
References
-
- Apfelbaum JL, Hagberg CA, Caplan RA, Blitt CD, Connis RT, Nickinovich DG, et al. Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology. 2013;118: 251–270. 10.1097/ALN.0b013e31827773b2 - DOI - PubMed
-
- Oshika H, Koyama Y, Taguri M, Maruyama K, Hirabayashi G, Yamada SM, et al. Supraglottic airway device versus a channeled or non-channeled blade-type videolaryngoscope for accidental extubation in the prone position: a randomized crossover manikin study. Medicine. 2018;97: e11190 10.1097/MD.0000000000011190 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
