

Lack of Humoral Immunity Against Glucosaminidase Is Associated with Postoperative Complications in Staphylococcus aureus Osteomyelitis
- PMID: 32858560
- PMCID: PMC9018051
- DOI: 10.2106/JBJS.20.00029
Lack of Humoral Immunity Against Glucosaminidase Is Associated with Postoperative Complications in Staphylococcus aureus Osteomyelitis
Abstract
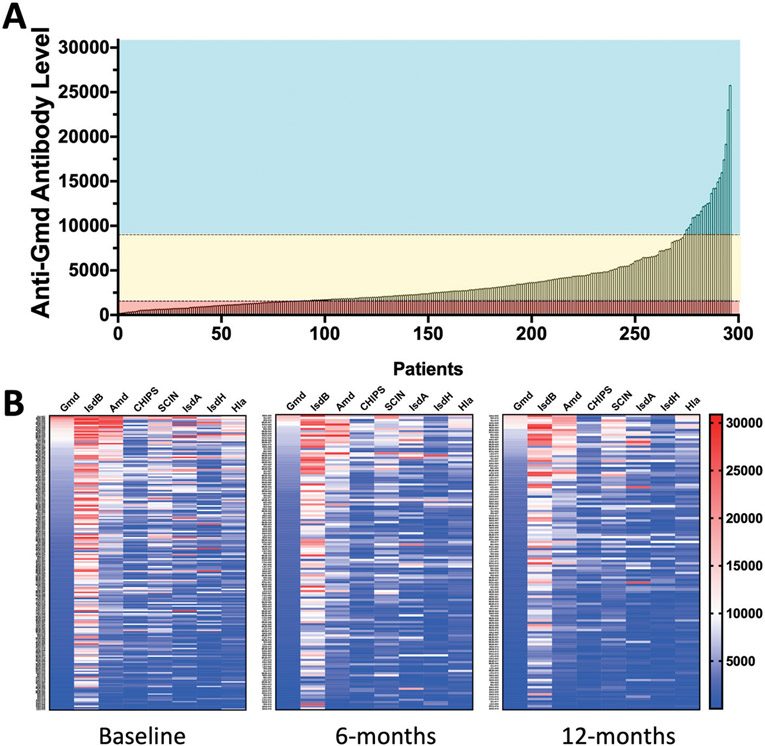
Background: Glucosaminidase (Gmd) is known to be a protective antigen in animal models of Staphylococcus aureus osteomyelitis. We compared the endogenous anti-Gmd antibody levels in sera of patients with culture-confirmed S. aureus bone infections to their sera at 1 year after operative treatment of the infection.
Methods: A novel global biospecimen registry of 297 patients with deep-wound culture-confirmed S. aureus osteomyelitis was analyzed to assess relationships between baseline anti-Gmd serum titers (via custom Luminex assay), known host risk factors for infection, and 1-year postoperative clinical outcomes (e.g., infection control, inconclusive, refracture, persistent infection, septic nonunion, amputation, and septic death).
Results: All patients had measurable humoral immunity against some S. aureus antigens, but only 20 patients (6.7%; p < 0.0001) had high levels of anti-Gmd antibodies (>10 ng/mL) in serum at baseline. A subset of 194 patients (65.3%) who completed 1 year of follow-up was divided into groups based on anti-Gmd level: low (<1 ng/mL, 54 patients; 27.8%), intermediate (<10 ng/mL, 122 patients; 62.9%), and high (>10 ng/mL, 18 patients; 9.3%), and infection control rates were 40.7%, 50.0%, and 66.7%, respectively. The incidence of adverse outcomes in these groups was 33.3%, 16.4%, and 11.1%, respectively. Assessing anti-Gmd level as a continuous variable showed a 60% reduction in adverse-event odds (p = 0.04) for every tenfold increase in concentration. No differences in patient demographics, body mass index of >40 kg/m, diabetes status, age of ≥70 years, male sex, Charlson Comorbidity Index of >1, or Cierny-Mader host type were observed between groups, and these risk factors were not associated with adverse events. Patients with low anti-Gmd titer demonstrated a significant 2.68-fold increased odds of adverse outcomes (p = 0.008).
Conclusions: Deficiency in circulating anti-Gmd antibodies was associated serious adverse outcomes following operative treatment of S. aureus osteomyelitis. At 1 year, high levels of anti-Gmd antibodies were associated with a nearly 3-fold increase in infection-control odds. Additional prospective studies clarifying Gmd immunization for osteomyelitis are needed.
Level of evidence: Prognostic Level IV. See Instructions for Authors for a complete description of levels of evidence.
Figures
Comment in
-
Searching for the Holy Grail of Infection Prevention: Commentary on an article by Stephen L. Kates, MD, et al.: "Lack of Humoral Immunity Against Glucosaminidase Is Associated with Postoperative Complications in Staphylococcus aureus Osteomyelitis".J Bone Joint Surg Am. 2020 Nov 4;102(21):e122. doi: 10.2106/JBJS.20.01581. J Bone Joint Surg Am. 2020. PMID: 33148957 No abstract available.
Similar articles
-
Evidence of Neutralizing and Non-Neutralizing Anti-Glucosaminidase Antibodies in Patients With S. Aureus Osteomyelitis and Their Association With Clinical Outcome Following Surgery in a Clinical Pilot.Front Cell Infect Microbiol. 2022 Jul 18;12:876898. doi: 10.3389/fcimb.2022.876898. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 35923804 Free PMC article.
-
Deriving a dose and regimen for anti-glucosaminidase antibody passive-immunisation for patients with Staphylococcus aureus osteomyelitis.Eur Cell Mater. 2020 Jan 31;39:96-107. doi: 10.22203/eCM.v039a06. Eur Cell Mater. 2020. PMID: 32003439 Free PMC article.
-
Anti-glucosaminidase IgG in sera as a biomarker of host immunity against Staphylococcus aureus in orthopaedic surgery patients.J Bone Joint Surg Am. 2013 Nov 20;95(22):e171. doi: 10.2106/JBJS.L.01654. J Bone Joint Surg Am. 2013. PMID: 24257671 Free PMC article.
-
Mechanisms of Immune Evasion and Bone Tissue Colonization That Make Staphylococcus aureus the Primary Pathogen in Osteomyelitis.Curr Osteoporos Rep. 2019 Dec;17(6):395-404. doi: 10.1007/s11914-019-00548-4. Curr Osteoporos Rep. 2019. PMID: 31721069 Free PMC article. Review.
-
Clinical and molecular aspects of the pathogenesis of Staphylococcus aureus bone and joint infections.J Med Microbiol. 1996 Mar;44(3):157-64. doi: 10.1099/00222615-44-3-157. J Med Microbiol. 1996. PMID: 8636931 Review.
Cited by
-
Evidence of Neutralizing and Non-Neutralizing Anti-Glucosaminidase Antibodies in Patients With S. Aureus Osteomyelitis and Their Association With Clinical Outcome Following Surgery in a Clinical Pilot.Front Cell Infect Microbiol. 2022 Jul 18;12:876898. doi: 10.3389/fcimb.2022.876898. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 35923804 Free PMC article.
-
Distinct expression trend of signature antigens of Staphylococcus aureus osteomyelitis correlated with clinical outcomes.J Orthop Res. 2021 Feb;39(2):265-273. doi: 10.1002/jor.24961. Epub 2020 Dec 29. J Orthop Res. 2021. PMID: 33336817 Free PMC article.
-
Skeletal infections: microbial pathogenesis, immunity and clinical management.Nat Rev Microbiol. 2022 Jul;20(7):385-400. doi: 10.1038/s41579-022-00686-0. Epub 2022 Feb 15. Nat Rev Microbiol. 2022. PMID: 35169289 Free PMC article. Review.
-
Staphylococcus aureus Cell Wall Biosynthesis Modulates Bone Invasion and Osteomyelitis Pathogenesis.Front Microbiol. 2021 Aug 16;12:723498. doi: 10.3389/fmicb.2021.723498. eCollection 2021. Front Microbiol. 2021. PMID: 34484165 Free PMC article.
-
IgG4-specific responses in patients with Staphylococcus aureus bone infections are not predictive of postoperative complications.Eur Cell Mater. 2021 Sep 22;42:156-165. doi: 10.22203/eCM.v042a12. Eur Cell Mater. 2021. PMID: 34549414 Free PMC article.
References
-
- Schwarz EM, Parvizi J, Gehrke T, Aiyer A, Battenberg A, Brown SA, Callaghan JJ, Citak M, Egol K, Garrigues GE, Ghert M, Goswami K, Green A, Hammound S, Kates SL, McLaren AC, Mont MA, Namdari S, Obremskey WT, O’Toole R, Raikin S, Restrepo C, Ricciardi B, Saeed K, Sanchez-Sotelo J, Shohat N, Tan T, Thirukumaran CP, Winters B. 2018 International Consensus Meeting on Musculoskeletal Infection: research priorities from the general assembly questions. J Orthop Res. 2019. May;37(5):997–1006. Epub 2019 Apr 25. - PubMed
-
- Darouiche RO. Treatment of infections associated with surgical implants. N Engl J Med. 2004. Apr 1;350(14):1422–9. - PubMed
-
- Kaplan SL. Recent lessons for the management of bone and joint infections. J Infect. 2014. Jan;68(Suppl 1):S51–6. Epub 2013 Oct 9. - PubMed
-
- Assis LM, Nedeljković M, Dessen A. New strategies for targeting and treatment of multi-drug resistant Staphylococcus aureus. Drug Resist Updat. 2017. Mar;31:1–14. Epub 2017 Apr 6. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
