

Maternal Oral Health Influences Infant Salivary Microbiome
- PMID: 32859139
- PMCID: PMC7755948
- DOI: 10.1177/0022034520947665
Maternal Oral Health Influences Infant Salivary Microbiome
Abstract
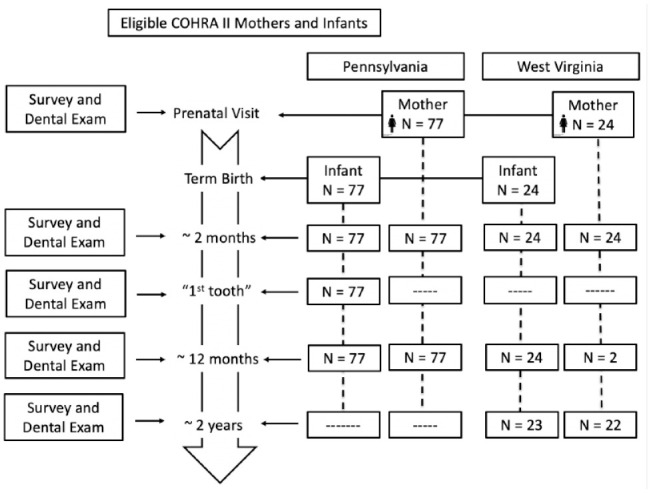
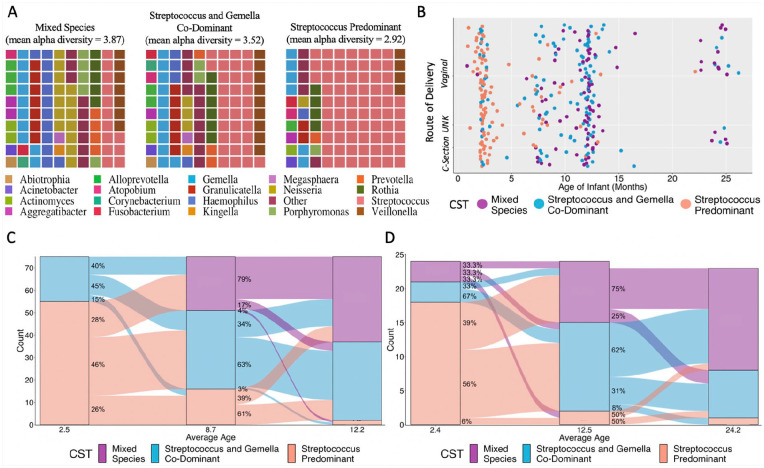
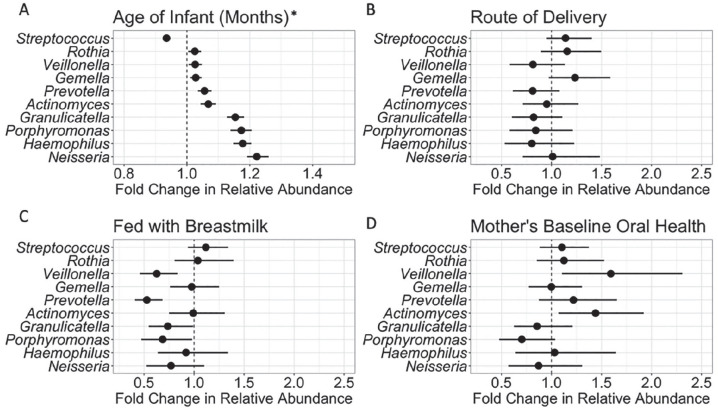
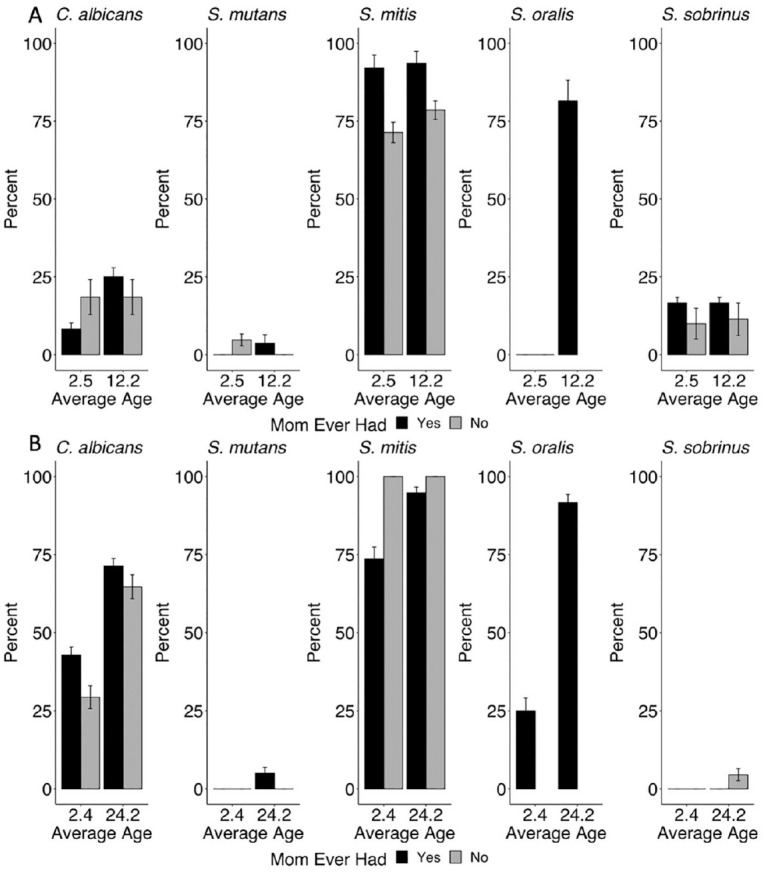
Oral microbiomes vary in cariogenic potential; these differences may be established early in life. A major concern is whether mothers transmit cariogenic bacteria to their children. Here we characterize early salivary microbiome development and the potential associations of that development with route of delivery, breastfeeding, and mother's oral health, and we evaluate transmission of microbes between mother and child. We analyzed saliva and metadata from the Center for Oral Health Research in Appalachia. For this cohort study, we sequenced the V6 region of the 16S rRNA gene and used quantitative polymerase chain reaction to detect Streptococcus mitis, Streptococcus sobrinus, Streptococcus mutans, Streptococcus oralis, and Candida albicans in the saliva from mothers and their infants, collected at 2, 9, and 12 mo (Pennsylvania site) and 2, 12, and 24 mo (West Virginia site). Breastfed children had lower relative abundances of Prevotella and Veillonella. If mothers had decayed, missing, or filled teeth, children had greater abundances of Veillonella and Actinomyces. There was little evidence of maternal transmission of selected microbes. At 12 mo, children's microbiomes were more similar to other children's than to their mothers'. Infants' salivary microbiomes became more adult-like with age but still differed with mothers' microbiomes at 12 mo. There was little evidence supporting transmission of selected microbes from mothers to children, but risk of colonization was associated with tooth emergence. Children are likely to acquire cariogenic bacteria from a variety of sources, including foods and contact with other children and adults.
Keywords: 16S rRNA; caries; early childhood caries; epidemiology; gingivitis; oral microbiome.
Conflict of interest statement
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
Figures
References
-
- Benjamini Y, Hochberg Y. 1995. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc Ser B. 57(1):289–300.
-
- Berkowitz RJ. 2003. Causes, treatment and prevention of early childhood caries: a microbiologic perspective. J Can Dent Assoc. 69(5):304–307. - PubMed
-
- Bertolini M, Dongari-Bagtzoglou A. 2019. The relationship of Candida albicans with the oral bacterial microbiome in health and disease. Adv Exp Med Biol. 1197:69–78. - PubMed
-
- De Abreu Da Silva Bastos V, Freitas-Fernandes LB, Da Silva Fidalgo TK, Martins C, Mattos CT, De Souza IPR, Maia LC. 2015. Mother-to-child transmission of Streptococcus mutans: a systematic review and meta-analysis. J Dent. 43(2):181–191. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
