

Lymphocyte Infiltration Determines the Hypoxia-Dependent Response to Definitive Chemoradiation in Head-and-Neck Cancer: Results from a Prospective Imaging Trial
- PMID: 32859699
- PMCID: PMC8049369
- DOI: 10.2967/jnumed.120.248633
Lymphocyte Infiltration Determines the Hypoxia-Dependent Response to Definitive Chemoradiation in Head-and-Neck Cancer: Results from a Prospective Imaging Trial
Abstract
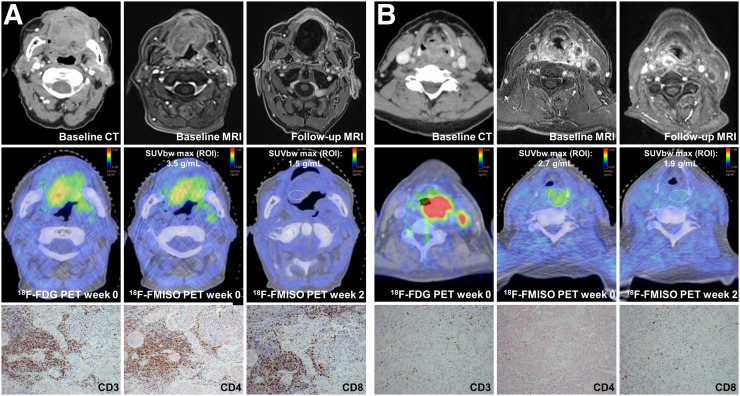
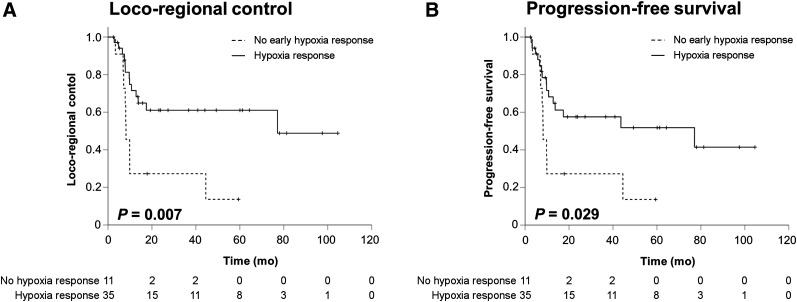
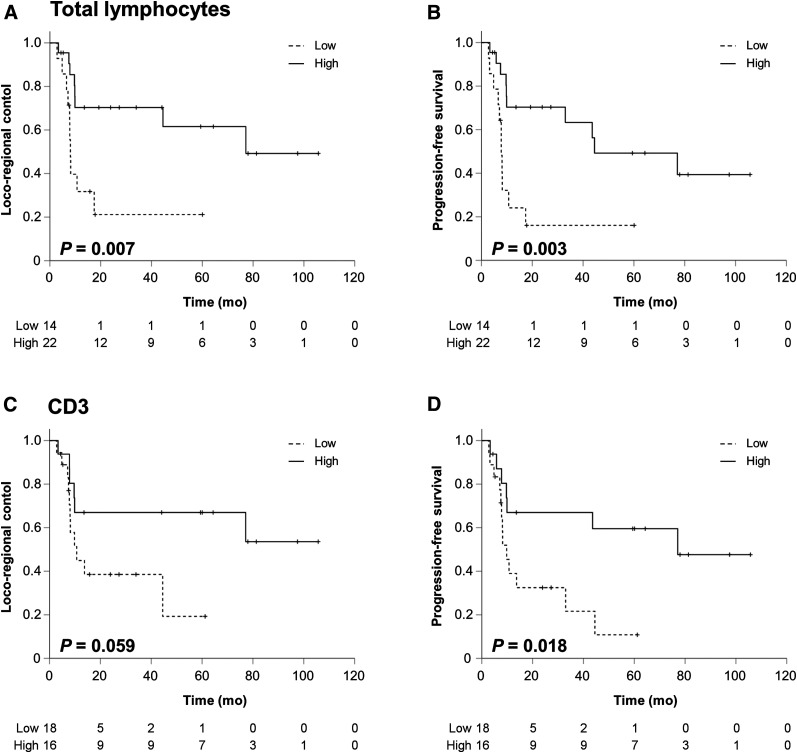
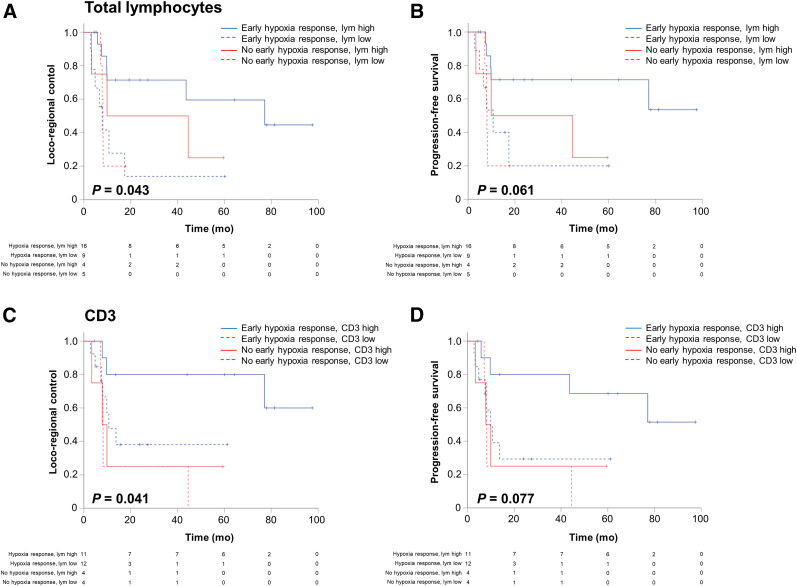
Tumor hypoxia in head-and-neck squamous cell carcinoma (HNSCC) leads to an immunosuppressive microenvironment and reduces the response to radiotherapy. In this prospective imaging trial, we investigated potential interactions between functional hypoxia imaging and infiltrating lymphocyte levels as a potential predictor for treatment response in HNSCC patients. Methods: In total, 49 patients receiving definitive chemoradiation for locally advanced HNSCCs underwent pretherapeutic biopsies and peritherapeutic hypoxia imaging using 18F-misonidazole PET at weeks 0, 2, and 5 during chemoradiation. Hematoxylin-eosin and immunohistochemical stainings for tumor-infiltrating lymphocytes, tissue-based hypoxia, and microvascular markers were analyzed and correlated with the longitudinal hypoxia dynamics and patient outcomes. Results: High levels of tumor-infiltrating total lymphocytes correlated with superior locoregional control (LRC) (hazard ratio [HR], 0.279; P = 0.011) and progression-free survival (PFS) (HR, 0.276; P = 0.006). Similarly, early resolution of 18F-misonidazole PET-detected tumor hypoxia quantified by 18F-misonidazole dynamics between weeks 0 and 2 of chemoradiation was associated with improved LRC (HR, 0.321; P = 0.015) and PFS (HR, 0.402; P = 0.043). Outcomes in the favorable early hypoxia resolution subgroup significantly depended on infiltrating lymphocyte counts, with patients who showed both an early hypoxia response and high lymphocyte infiltration levels exhibiting significantly improved LRC (HR, 0.259; P = 0.036) and PFS (HR, 0.242; P = 0.017) compared with patients with an early hypoxia response but low lymphocyte counts. These patients exhibited oncologic results comparable to those of patients with no hypoxia response within the first 2 wk of chemoradiation. Conclusion: This analysis established a clinical hypoxia-immune score that predicted treatment responses and outcomes in HNSCC patients undergoing chemoradiation and may help to devise novel concepts for biology-driven personalization of chemoradiation.
Keywords: FMISO PET; chemoradiation; head-and-neck cancer; hypoxia; immune system.
© 2021 by the Society of Nuclear Medicine and Molecular Imaging.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Blanchard P, Baujat B, Holostenco V, et al. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): a comprehensive analysis by tumour site. Radiother Oncol. 2011;100:33–40. - PubMed
-
- Baumann R, Depping R, Delaperriere M, Dunst J. Targeting hypoxia to overcome radiation resistance in head & neck cancers: real challenge or clinical fairytale? Expert Rev Anticancer Ther. 2016;16:751–758. - PubMed
-
- Overgaard J, Eriksen JG, Nordsmark M, Alsner J, Horsman MR. Plasma osteopontin, hypoxia, and response to the hypoxia sensitiser nimorazole in radiotherapy of head and neck cancer: results from the DAHANCA 5 randomised double-blind placebo-controlled trial. Lancet Oncol. 2005;6:757–764. - PubMed
-
- Mortensen LS, Johansen J, Kallehauge J, et al. FAZA PET/CT hypoxia imaging in patients with squamous cell carcinoma of the head and neck treated with radiotherapy: results from the DAHANCA 24 trial. Radiother Oncol. 2012;105:14–20. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical