

Comparison of 68Ga-DOTANOC with 18F-FDG using PET/MRI imaging in patients with pulmonary tuberculosis
- PMID: 32859979
- PMCID: PMC7455716
- DOI: 10.1038/s41598-020-71127-2
Comparison of 68Ga-DOTANOC with 18F-FDG using PET/MRI imaging in patients with pulmonary tuberculosis
Abstract
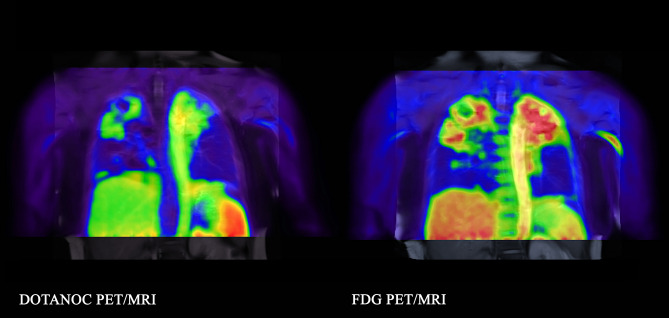
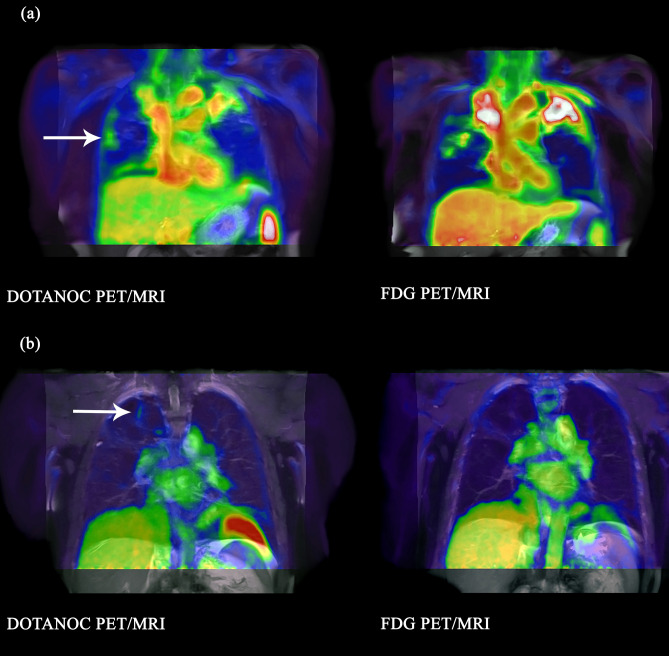
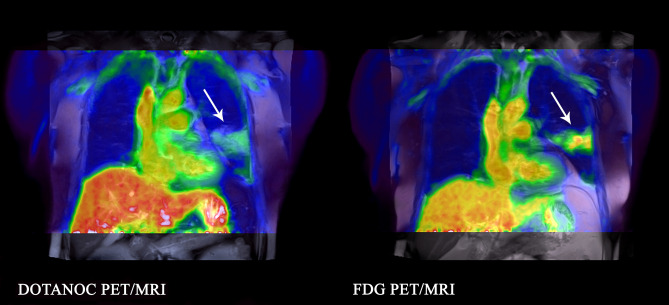
We compared the somatostatin analog radioligand, DOTANOC, with FDG, to determine whether there was increased detection of active or sub-clinical lesions in pulmonary tuberculosis (TB) with DOTANOC. Three groups were recruited: (1) active pulmonary TB; (2) IGRA-positive household TB contacts; (3) pneumonia (non-TB). DOTANOC PET/MRI followed by FDG PET/MRI was performed in active TB and pneumonia groups. TB contacts underwent FDG PET/MRI, then DOTANOC PET/MRI if abnormalities were detected. Quantitative and qualitative analyses were performed for total lung and individual lesions. Eight active TB participants, three TB contacts and three pneumonia patients had paired PET/MRI scans. In the active TB group, median SUVmax[FDG] for parenchymal lesions was 7.69 (range 3.00-15.88); median SUVmax[DOTANOC] was 2.59 (1.48-6.40). Regions of tracer uptake were fairly similar for both radioligands, albeit more diffusely distributed in the FDG scans. In TB contacts, two PET/MRIs had parenchymal lesions detected with FDG (SUVmax 5.50 and 1.82), with corresponding DOTANOC uptake < 1. FDG and DOTANOC uptake was similar in pneumonia patients (SUVmax[FDG] 4.17-6.18; SUVmax[DOTANOC] 2.92-4.78). DOTANOC can detect pulmonary TB lesions, but FDG is more sensitive for both active and sub-clinical lesions. FDG remains the preferred ligand for clinical studies, although DOTANOC may provide additional value for pathogenesis studies.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- World Health Organisation. Global tuberculosis report 2019. https://apps.who.int/iris/bitstream/handle/10665/329368/9789241565714-en... (2019).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
