

Successful application of genome sequencing in a diagnostic setting: 1007 index cases from a clinically heterogeneous cohort
- PMID: 32860008
- PMCID: PMC7852664
- DOI: 10.1038/s41431-020-00713-9
Successful application of genome sequencing in a diagnostic setting: 1007 index cases from a clinically heterogeneous cohort
Abstract
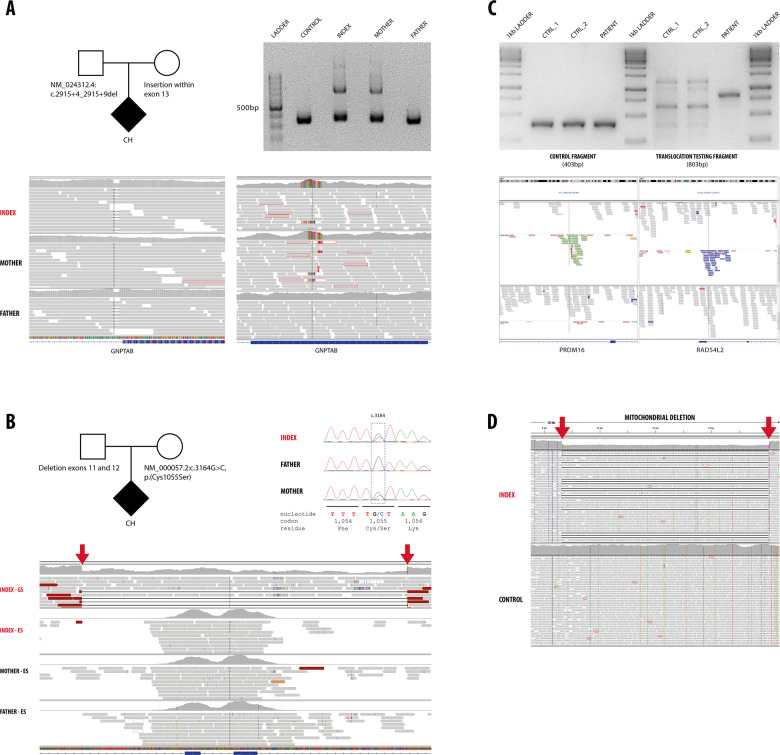
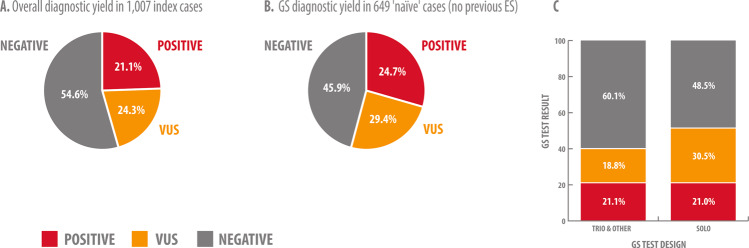
Despite clear technical superiority of genome sequencing (GS) over other diagnostic methods such as exome sequencing (ES), few studies are available regarding the advantages of its clinical application. We analyzed 1007 consecutive index cases for whom GS was performed in a diagnostic setting over a 2-year period. We reported pathogenic and likely pathogenic (P/LP) variants that explain the patients' phenotype in 212 of the 1007 cases (21.1%). In 245 additional cases (24.3%), a variant of unknown significance (VUS) related to the phenotype was reported. We especially investigated patients which had had ES with no genetic diagnosis (n = 358). For this group, GS diagnostic yield was 14.5% (52 patients with P/LP out of 358). GS should be especially indicated for ES-negative cases since up to 29.6% of them could benefit from GS testing (14.5% with P/LP, n = 52 and 15.1% with VUS, n = 54). Genetic diagnoses in most of the ES-negative/GS-positive cases were determined by technical superiority of GS, i.e., access to noncoding regions and more uniform coverage. Importantly, we reported 79 noncoding variants, of which, 41 variants were classified as P/LP. Interpretation of noncoding variants remains challenging, and in many cases, complementary methods based on direct enzyme assessment, biomarker testing and RNA analysis are needed for variant classification and diagnosis. We present the largest cohort of patients with GS performed in a clinical setting to date. The results of this study should direct the decision for GS as standard second-line, or even first-line stand-alone test.
Conflict of interest statement
AMB-A, CB, NA, MER, PG, CP, NO, KKK, MW, OP, SZ, DU, GW, KK, FV, AR and PB are current or former (MSC, MC, DDA, MZ) employees at CENTOGENE, AG. None of the other authors declared a potential conflict of interest.
Figures
Comment in
-
The question of WGS's clinical utility remains unanswered.Eur J Hum Genet. 2021 May;29(5):722-723. doi: 10.1038/s41431-021-00823-y. Epub 2021 Feb 17. Eur J Hum Genet. 2021. PMID: 33597733 Free PMC article. No abstract available.
-
Reply letter to Battke et al.Eur J Hum Genet. 2021 May;29(5):724-725. doi: 10.1038/s41431-021-00819-8. Epub 2021 Feb 17. Eur J Hum Genet. 2021. PMID: 33597734 Free PMC article. No abstract available.
References
-
- Farwell KD, Shahmirzadi L, El-Khechen D, Powis Z, Chao EC, Tippin Davis B, et al. Enhanced utility of family-centered diagnostic exome sequencing with inheritance model-based analysis: results from 500 unselected families with undiagnosed genetic conditions. Genet Med. 2015;17:578–86. doi: 10.1038/gim.2014.154. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
