

Effect of icosapent ethyl on progression of coronary atherosclerosis in patients with elevated triglycerides on statin therapy: final results of the EVAPORATE trial
- PMID: 32860032
- PMCID: PMC7654934
- DOI: 10.1093/eurheartj/ehaa652
Effect of icosapent ethyl on progression of coronary atherosclerosis in patients with elevated triglycerides on statin therapy: final results of the EVAPORATE trial
Abstract
Aims: Despite the effects of statins in reducing cardiovascular events and slowing progression of coronary atherosclerosis, significant cardiovascular (CV) risk remains. Icosapent ethyl (IPE), a highly purified eicosapentaenoic acid ethyl ester, added to a statin was shown to reduce initial CV events by 25% and total CV events by 32% in the REDUCE-IT trial, with the mechanisms of benefit not yet fully explained. The EVAPORATE trial sought to determine whether IPE 4 g/day, as an adjunct to diet and statin therapy, would result in a greater change from baseline in plaque volume, measured by serial multidetector computed tomography (MDCT), than placebo in statin-treated patients.
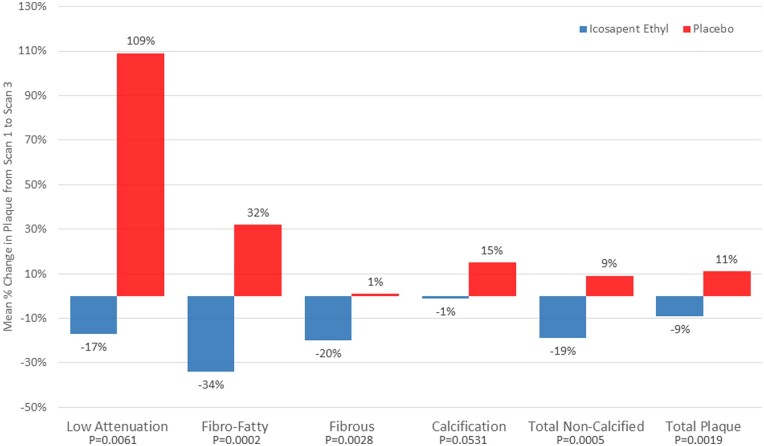
Methods and results: A total of 80 patients were enrolled in this randomized, double-blind, placebo-controlled trial. Patients had to have coronary atherosclerosis as documented by MDCT (one or more angiographic stenoses with ≥20% narrowing), be on statin therapy, and have persistently elevated triglyceride (TG) levels. Patients underwent an interim scan at 9 months and a final scan at 18 months with coronary computed tomographic angiography. The pre-specified primary endpoint was change in low-attenuation plaque (LAP) volume at 18 months between IPE and placebo groups. Baseline demographics, vitals, and laboratory results were not significantly different between the IPE and placebo groups; the median TG level was 259.1 ± 78.1 mg/dL. There was a significant reduction in the primary endpoint as IPE reduced LAP plaque volume by 17%, while in the placebo group LAP plaque volume more than doubled (+109%) (P = 0.0061). There were significant differences in rates of progression between IPE and placebo at study end involving other plaque volumes including fibrous, and fibrofatty (FF) plaque volumes which regressed in the IPE group and progressed in the placebo group (P < 0.01 for all). When further adjusted for age, sex, diabetes status, hypertension, and baseline TG, plaque volume changes between groups remained significantly different, P < 0.01. Only dense calcium did not show a significant difference between groups in multivariable modelling (P = 0.053).
Conclusions: Icosapent ethyl demonstrated significant regression of LAP volume on MDCT compared with placebo over 18 months. EVAPORATE provides important mechanistic data on plaque characteristics that may have relevance to the REDUCE-IT results and clinical use of IPE.
Keywords: Atherosclerosis; Cardiac CT; Coronary artery disease; Prevention; Progression.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Can EPA evaporate plaques?Eur Heart J. 2020 Oct 21;41(40):3933-3935. doi: 10.1093/eurheartj/ehaa750. Eur Heart J. 2020. PMID: 33141163 No abstract available.
-
The EVAPORATE trial provides important mechanistic data on plaque characteristics that have relevance to the REDUCE-IT results and clinical use of icosapent ethyl.Eur Heart J. 2021 Aug 17;42(31):3025-3026. doi: 10.1093/eurheartj/ehab233. Eur Heart J. 2021. PMID: 33970207 No abstract available.
-
Underlying mechanisms involved in the icosapent ethyl reduction of cardiovascular events still cannot be attributed to an anti-atherosclerotic effect.Eur Heart J. 2021 Aug 17;42(31):3023-3024. doi: 10.1093/eurheartj/ehab230. Eur Heart J. 2021. PMID: 33970235 No abstract available.
References
-
- Fan W, Philip S, Granowitz C, Toth PP, Wong ND. Hypertriglyceridemia in statin-treated US adults: the National Health and Nutrition Examination Survey. J Clin Lipidol 2019;13:100–108. - PubMed
-
- Bhatt DL, Steg PG, Miller M, Brinton EA, Jacobson TA, Ketchum SB, Doyle RT, Juliano RA, Jiao L, Granowitz C, Tardif J-C, Ballantyne CM; REDUCE-IT Investigators. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med 2019;380:11–22. - PubMed
-
- Bhatt DL, Steg PG, Miller M, Brinton EA, Jacobson TA, Ketchum SB, Doyle RT, Juliano RA, Jiao L, Granowitz C, Tardif J-C, Gregson J, Pocock SJ, Ballantyne CM ; REDUCE-IT Investigators. Effects of icosapent ethyl on total ischemic events: from REDUCE-IT. J Am Coll Cardiol 2019;73:2791–2802. - PubMed
-
- Yokoyama M, Origasa H, Matsuzaki M, Matsuzawa Y, Saito Y, Ishikawa Y, Oikawa S, Sasaki J, Hishida H, Itakura H, Kita T, Kitabatake A, Nakaya N, Sakata T, Shimada K, Shirato K; Japan EPA lipid intervention study (JELIS) Investigators. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis. Lancet (London, England) 2007;369:1090–1098. - PubMed
-
- Patel AA, Budoff MJ. Effects of eicosapentaenoic acid and docosahexaenoic acid on lipoproteins in hypertriglyceridemia. Curr Opin Endocrinol Diabetes Obes 2016;23:145–149. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
