

Time-to-treatment initiation of colchicine and cardiovascular outcomes after myocardial infarction in the Colchicine Cardiovascular Outcomes Trial (COLCOT)
- PMID: 32860034
- PMCID: PMC7700755
- DOI: 10.1093/eurheartj/ehaa659
Time-to-treatment initiation of colchicine and cardiovascular outcomes after myocardial infarction in the Colchicine Cardiovascular Outcomes Trial (COLCOT)
Abstract
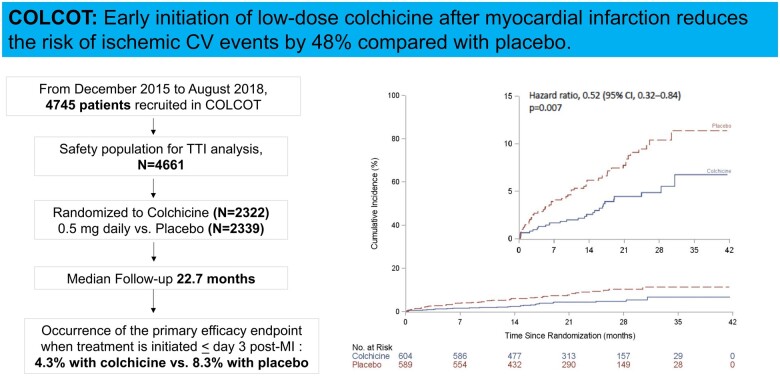
Aims: The COLchicine Cardiovascular Outcomes Trial (COLCOT) demonstrated the benefits of targeting inflammation after myocardial infarction (MI). We aimed to determine whether time-to-treatment initiation (TTI) influences the beneficial impact of colchicine.
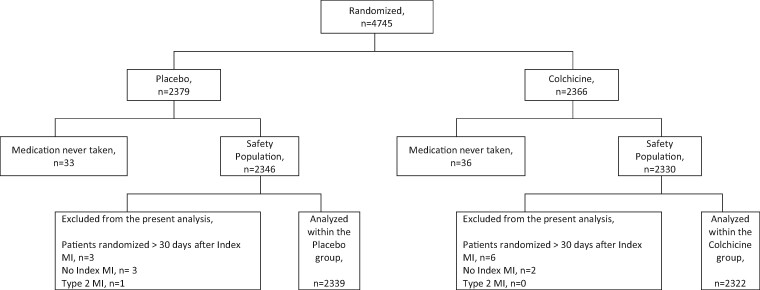
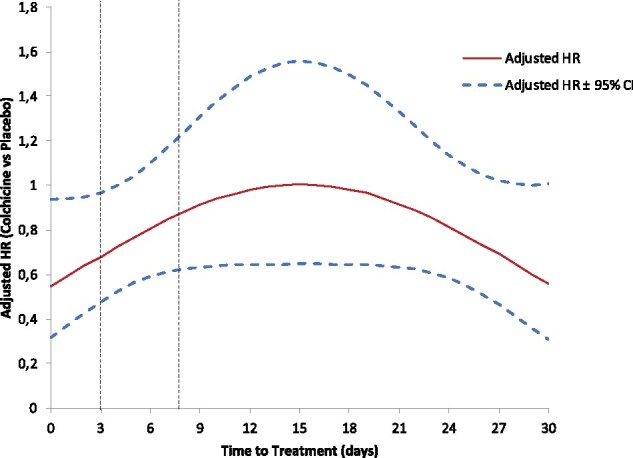
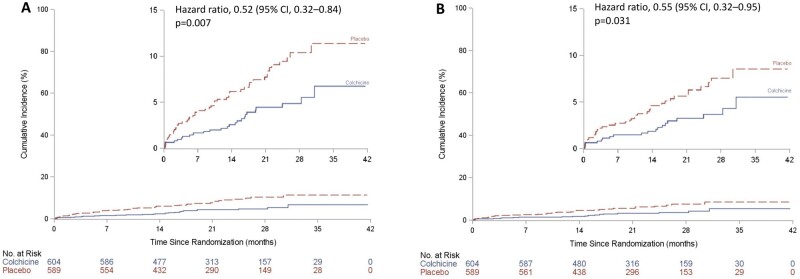
Methods and results: In COLCOT, patients were randomly assigned to receive colchicine or placebo within 30 days post-MI. Time-to-treatment initiation was defined as the length of time between the index MI and the initiation of study medication. The primary efficacy endpoint was a composite of cardiovascular death, resuscitated cardiac arrest, MI, stroke, or urgent hospitalization for angina requiring coronary revascularization. The relationship between endpoints and various TTI (<3, 4-7 and >8 days) was examined using multivariable Cox regression models. Amongst the 4661 patients included in this analysis, there were 1193, 720, and 2748 patients, respectively, in the three TTI strata. After a median follow-up of 22.7 months, there was a significant reduction in the incidence of the primary endpoint for patients in whom colchicine was initiated < Day 3 compared with placebo [hazard ratios (HR) = 0.52, 95% confidence intervals (CI) 0.32-0.84], in contrast to patients in whom colchicine was initiated between Days 4 and 7 (HR = 0.96, 95% CI 0.53-1.75) or > Day 8 (HR = 0.82, 95% CI 0.61-1.11). The beneficial effects of early initiation of colchicine were also demonstrated for urgent hospitalization for angina requiring revascularization (HR = 0.35), all coronary revascularization (HR = 0.63), and the composite of cardiovascular death, resuscitated cardiac arrest, MI, or stroke (HR = 0.55, all P < 0.05).
Conclusion: Patients benefit from early, in-hospital initiation of colchicine after MI.
Trial registration: COLCOT ClinicalTrials.gov number, NCT02551094.
Keywords: COLCOT; Cardiovascular inflammation; Colchicine; Inflammasome; Time-to-treatment initiation.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
The sooner, the better: anti-inflammation in acute myocardial infarction.Eur Heart J. 2020 Nov 7;41(42):4100-4102. doi: 10.1093/eurheartj/ehaa752. Eur Heart J. 2020. PMID: 33249465 No abstract available.
-
Colchicine administered early in acute myocardial infarction: ready, set … go?Eur Heart J. 2021 Jul 21;42(28):2802. doi: 10.1093/eurheartj/ehab010. Eur Heart J. 2021. PMID: 33480985 No abstract available.
-
Lessons from COLCOT and LoDoCo2: colchicine for secondary prevention in coronary artery disease.Eur Heart J. 2021 Jul 21;42(28):2800-2801. doi: 10.1093/eurheartj/ehab020. Eur Heart J. 2021. PMID: 33496313 No abstract available.
-
Colchicine and coronary artery disease: a virtuous adoption.Eur Heart J. 2021 Jul 21;42(28):2796-2797. doi: 10.1093/eurheartj/ehab008. Eur Heart J. 2021. PMID: 33496321 No abstract available.
-
Initiation of low-dose colchicine early after myocardial infarction.Eur Heart J. 2021 Jul 21;42(28):2798-2799. doi: 10.1093/eurheartj/ehab038. Eur Heart J. 2021. PMID: 33537713 No abstract available.
References
-
- Liuzzo G, Biasucci LM, Gallimore JR, Grillo RL, Rebuzzi AG, Pepys MB, Maseri A. The prognostic value of C-reactive protein and serum amyloid a protein in severe unstable angina. N Engl J Med 1994;331:417–424. - PubMed
-
- Kawaguchi M, Takahashi M, Hata T, Kashima Y, Usui F, Morimoto H, Izawa A, Takahashi Y, Masumoto J, Koyama J, Hongo M, Noda T, Nakayama J, Sagara J, Taniguchi S, Ikeda U. Inflammasome activation of cardiac fibroblasts is essential for myocardial ischemia/reperfusion injury. Circulation 2011;123:594–604. - PubMed
-
- Westman PC, Lipinski MJ, Luger D, Waksman R, Bonow RO, Wu E, Epstein SE. Inflammation as a driver of adverse left ventricular remodeling after acute myocardial infarction. J Am Coll Cardiol 2016;67:2050–2060. - PubMed
-
- Chen B, Frangogiannis NG. Immune cells in repair of the infarcted myocardium. Microcirculation 2017;24:e12305. - PubMed
-
- Gao R, Shi H, Chang S, Gao Y, Li X, Lv C, Yang H, Xiang H, Yang J, Xu L, Tang Y. The selective NLRP3-inflammasome inhibitor MCC950 reduces myocardial fibrosis and improves cardiac remodeling in a mouse model of myocardial infarction. Int Immunopharmacol 2019;74:105575. - PubMed
