

Optimising the outcomes of index admission laparoscopic cholecystectomy and bile duct exploration for biliary emergencies: a service model
- PMID: 32860135
- PMCID: PMC8263394
- DOI: 10.1007/s00464-020-07900-1
Optimising the outcomes of index admission laparoscopic cholecystectomy and bile duct exploration for biliary emergencies: a service model
Abstract
Aims: The rate of acute laparoscopic cholecystectomy remains low due to operational constraints. The purpose of this study is to evaluate a service model of index admission cholecystectomy with referral protocols, refined logistics and targeted job planning.
Methods: A prospectively maintained dataset was evaluated to determine the processes of care and outcomes of patients undergoing emergency biliary surgery. The lead author has maintained a 28 years prospective database capturing standard demographic data, intraoperative details including the difficulty of cholecystectomy as well as postoperative outcome parameters and follow up data.
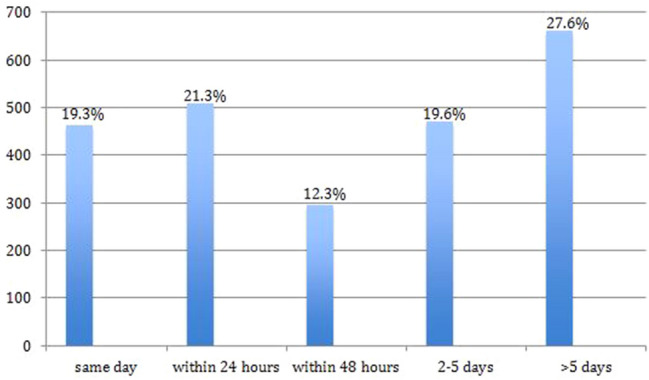
Results: Over five thousand (5555) consecutive laparoscopic cholecystectomies were performed. Only patients undergoing emergency procedures (2399,43.2% of entire group) were analysed for this study. The median age was 52 years with 70% being female. The majority were admitted with biliary pain (34%), obstructive jaundice (26%) and acute cholecystitis (16%). 63% were referred by other surgeons. 80% underwent surgery within 5 days (40% within 24 h). Cholecystectomies were performed on scheduled lists (44%) or dedicated emergency lists (29%). Two thirds had suspected bile duct stones and 38.1% underwent bile duct exploration. The median operating time was 75 min, median hospital stay 7 days, conversion rate 0.8%, morbidity 8.9% and mortality rate 0.2%.
Conclusion: Index admission cholecystectomy for biliary emergencies can have low rates of morbidity and mortality. Timely referral and flexible theatre lists facilitate the service, optimising clinical results, number of biliary episodes, hospital stay and presentation to resolution intervals. Cost benefits and reduced interval readmissions need to be weighed against the length of hospital stay per episode.
Keywords: Biliary emergencies; Difficulty grading; Emergency surgery; Gall stones; Index admission surgery; Laparoscopic cholecystectomy; Nassar Scale.
Conflict of interest statement
Ahmad H. M. Nassar, Hwei J. Ng, Zubir Ahmed, Arkadiusz Peter Wysocki, Colin Wood and Ayman Abdellatif have no conflicts of interest or financial ties to disclose.
Figures
References
-
- Hospital Episode Statistics Admitted Patient Care England (2013–2014) Health and Social Care Information Centre. https://www.hscic.gov.uk/catalogue/PUB16719. Accessed April 2020
-
- AUGIS/ASGBI J (2015) Pathway on management of acute gallstone diseases. https://www.augis.org/wp-content/uploads/2014/05/Acute-Gallstones-Pathwa.... Accessed April 2020
