

A Prognostic Gene-Expression Signature and Risk Score for Meningioma Recurrence After Resection
- PMID: 32860417
- PMCID: PMC7735867
- DOI: 10.1093/neuros/nyaa355
A Prognostic Gene-Expression Signature and Risk Score for Meningioma Recurrence After Resection
Abstract
Background: Prognostic markers for meningioma are needed to risk-stratify patients and guide postoperative surveillance and adjuvant therapy.
Objective: To identify a prognostic gene signature for meningioma recurrence and mortality after resection using targeted gene-expression analysis.
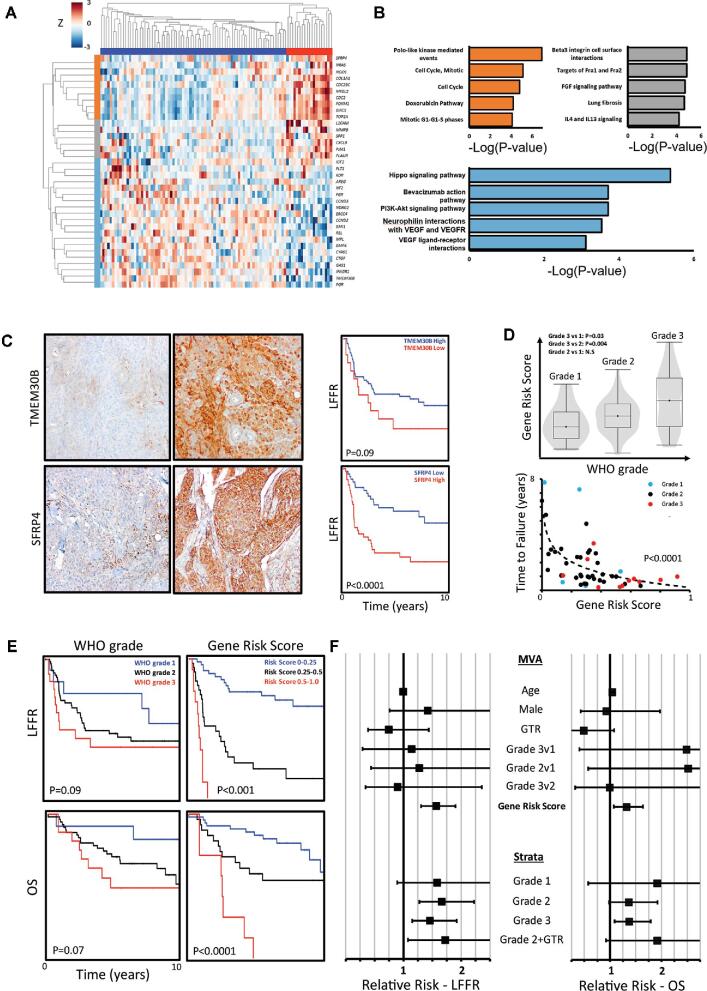
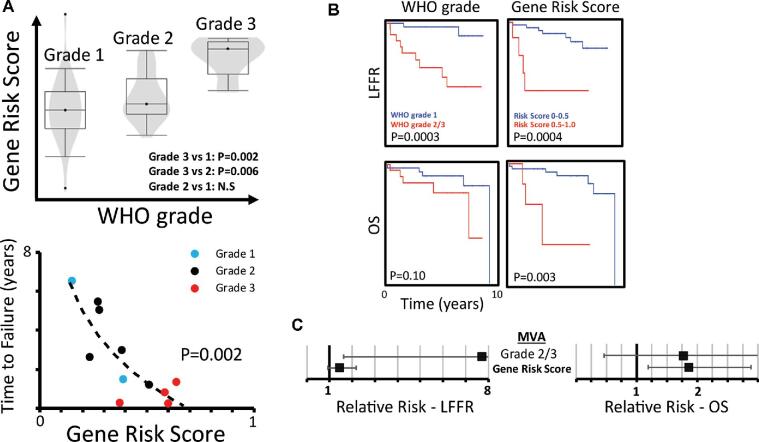
Methods: Targeted gene-expression analysis was used to interrogate a discovery cohort of 96 meningiomas and an independent validation cohort of 56 meningiomas with comprehensive clinical follow-up data from separate institutions. Bioinformatic analysis was used to identify prognostic genes and generate a gene-signature risk score between 0 and 1 for local recurrence.
Results: We identified a 36-gene signature of meningioma recurrence after resection that achieved an area under the curve of 0.86 in identifying tumors at risk for adverse clinical outcomes. The gene-signature risk score compared favorably to World Health Organization (WHO) grade in stratifying cases by local freedom from recurrence (LFFR, P < .001 vs .09, log-rank test), shorter time to failure (TTF, F-test, P < .0001), and overall survival (OS, P < .0001 vs .07) and was independently associated with worse LFFR (relative risk [RR] 1.56, 95% CI 1.30-1.90) and OS (RR 1.32, 95% CI 1.07-1.64), after adjusting for clinical covariates. When tested on an independent validation cohort, the gene-signature risk score remained associated with shorter TTF (F-test, P = .002), compared favorably to WHO grade in stratifying cases by OS (P = .003 vs P = .10), and was significantly associated with worse OS (RR 1.86, 95% CI 1.19-2.88) on multivariate analysis.
Conclusion: The prognostic meningioma gene-expression signature and risk score presented may be useful for identifying patients at risk for recurrence.
Keywords: Biomarker; Expression; Gene; Gene expression; Meningioma; Prognostic; Radiation; Recurrence; Resection; Survival; WHO grade.
Copyright © 2020 by the Congress of Neurological Surgeons.
Figures
References
-
- Aizer AA, Bi WL, Kandola MS et al. . Extent of resection and overall survival for patients with atypical and malignant meningioma. Cancer. 2015;121(24):4376-4378. - PubMed
-
- Chen WC, Magill ST, Wu A et al. . Histopathologic features predictive of local control of atypical meningioma after surgery and adjuvant radiotherapy. J Neurosurg. 2018;130(2):443-450. - PubMed
-
- Condra KS, Buatti JM, Mendenhall WM, Friedman WA, Marcus RB, Rhoton AL. Benign meningiomas: primary treatment selection affects survival. Int J Radiat Oncol Biol Phys. 1997;39(2):427-36. - PubMed
