

Effect of collaborative care between traditional and faith healers and primary health-care workers on psychosis outcomes in Nigeria and Ghana (COSIMPO): a cluster randomised controlled trial
- PMID: 32861306
- PMCID: PMC8473710
- DOI: 10.1016/S0140-6736(20)30634-6
Effect of collaborative care between traditional and faith healers and primary health-care workers on psychosis outcomes in Nigeria and Ghana (COSIMPO): a cluster randomised controlled trial
Abstract
Background: Traditional and faith healers (TFH) provide care to a large number of people with psychosis in many sub-Saharan African countries but they practise outside the formal mental health system. We aimed to assess the effectiveness and cost-effectiveness of a collaborative shared care model for psychosis delivered by TFH and primary health-care providers (PHCW).
Methods: In this cluster-randomised trial in Kumasi, Ghana and Ibadan, Nigeria, we randomly allocated clusters (a primary care clinic and neighbouring TFH facilities) 1:1, stratified by size and country, to an intervention group or enhanced care as usual. The intervention included a manualised collaborative shared care delivered by trained TFH and PHCW. Eligible participants were adults (aged ≥18 years) newly admitted to TFH facilities with active psychotic symptoms (positive and negative syndrome scale [PANSS] score ≥60). The primary outcome, by masked assessments at 6 months, was the difference in psychotic symptom improvement as measured with the PANSS in patients in follow-up at 3 and 6 months. Patients exposure to harmful treatment practices, such as shackling, were also assessed at 3 and 6 months. Care costs were assessed at baseline, 3-month and 6-month follow-up, and for the entire 6 months of follow-up. This trial was registered with the National Institutes of Health Clinical Trial registry, NCT02895269.
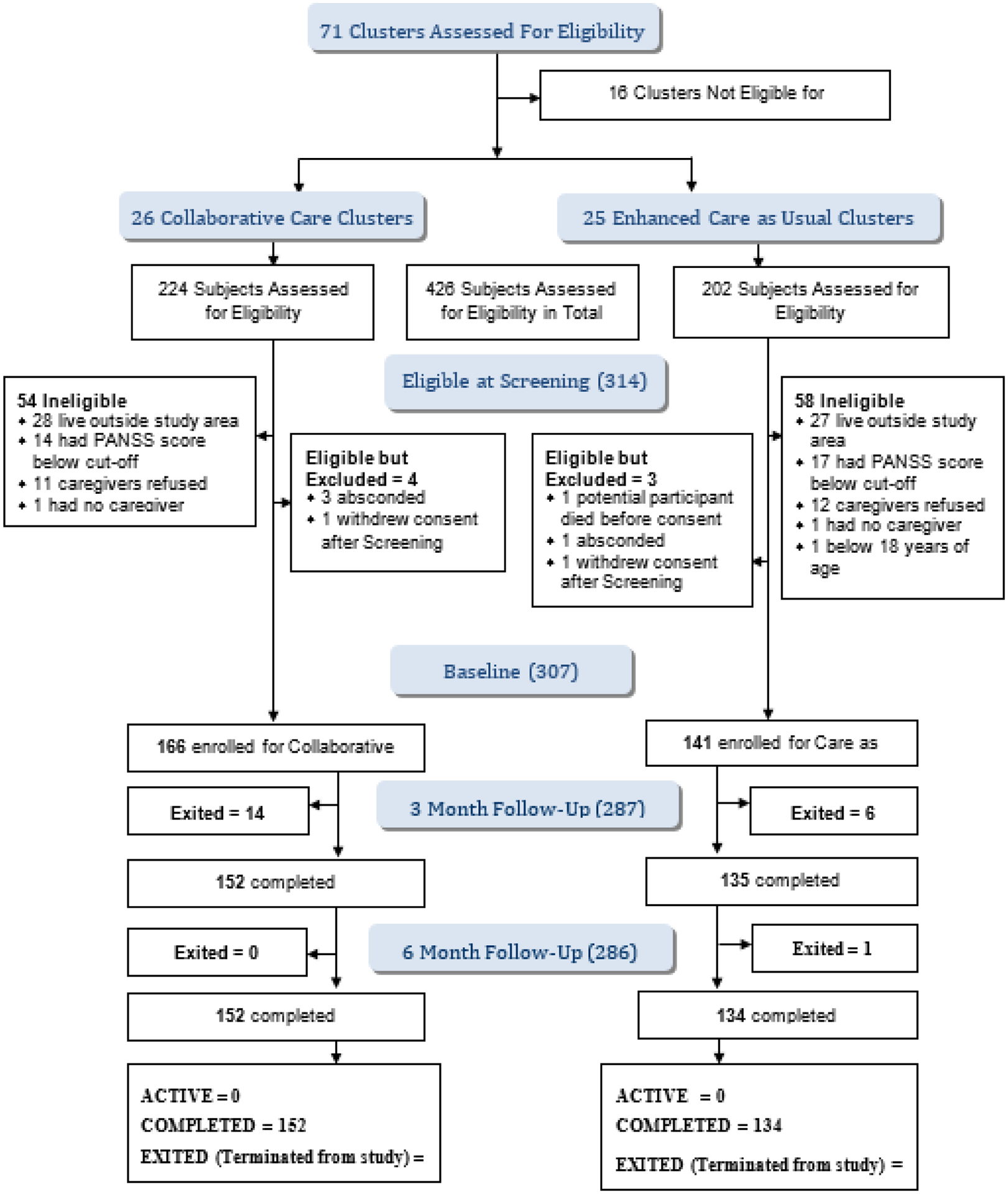
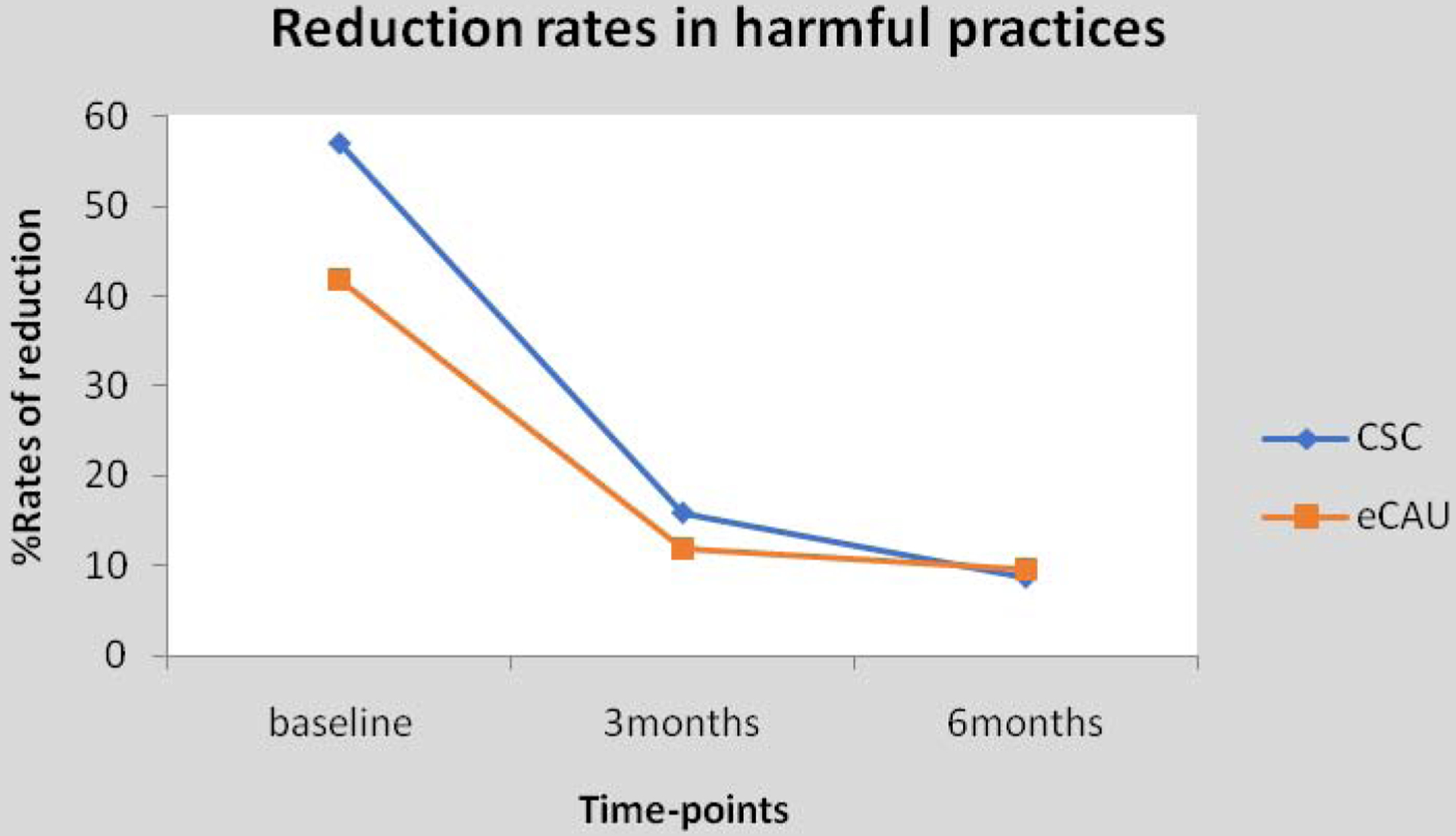
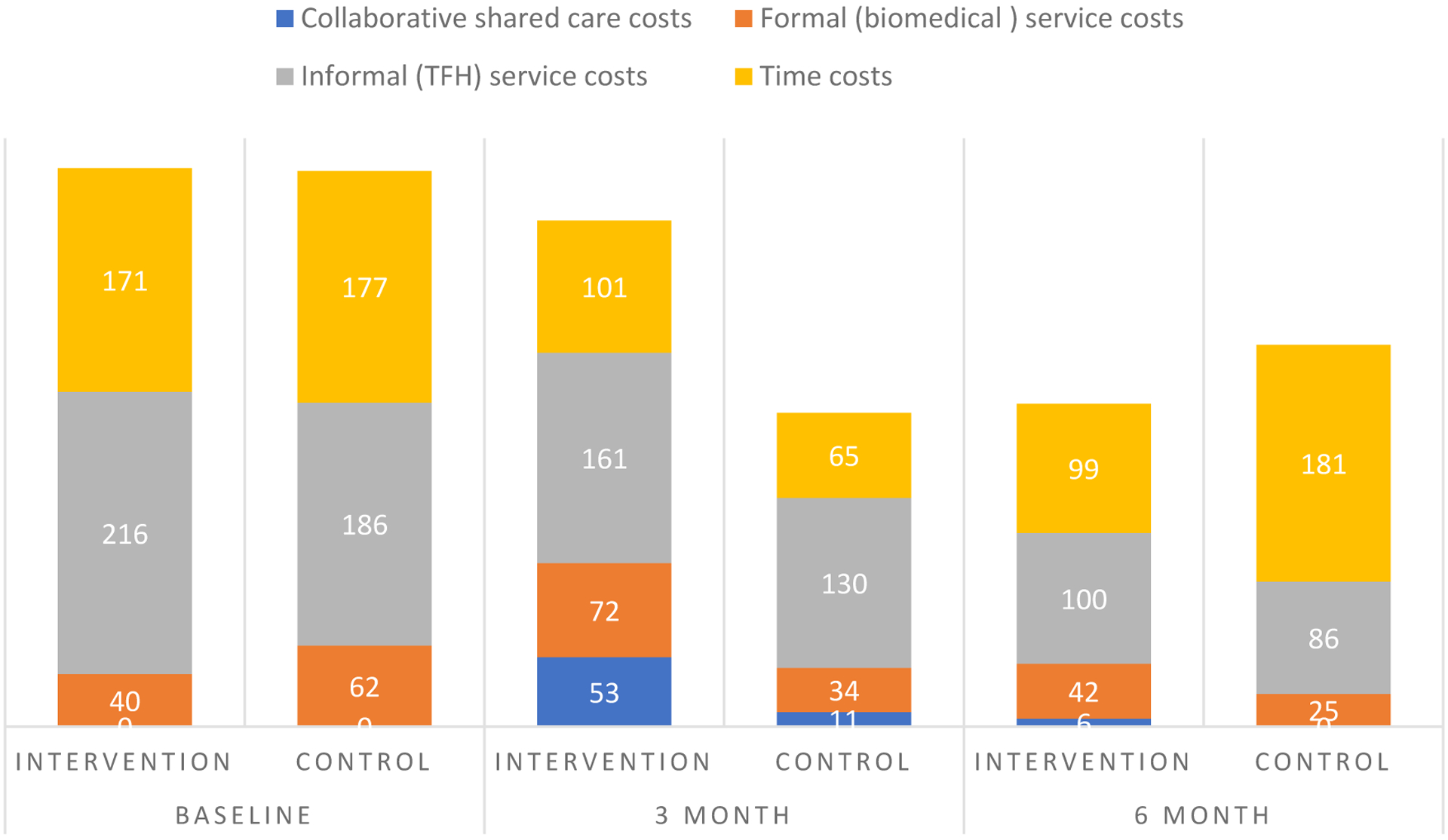
Findings: Between Sept 1, 2016, and May 3, 2017, 51 clusters were randomly allocated (26 intervention, 25 control) with 307 patients enrolled (166 [54%] in the intervention group and 141 [46%] in the control group). 190 (62%) of participants were men. Baseline mean PANSS score was 107·3 (SD 17·5) for the intervention group and 108·9 (18·3) for the control group. 286 (93%) completed the 6-month follow-up at which the mean total PANSS score for intervention group was 53·4 (19·9) compared with 67·6 (23·3) for the control group (adjusted mean difference -15·01 (95% CI -21·17 to -8·84; 0·0001). Harmful practices decreased from 94 (57%) of 166 patients at baseline to 13 (9%) of 152 at 6 months in the intervention group (-0·48 [-0·60 to -0·37] p<0·001) and from 59 (42%) of 141 patients to 13 (10%) of 134 in the control group (-0·33 [-0·45 to -0·21] p<0·001), with no significant difference between the two groups. Greater reductions in overall care costs were seen in the intervention group than in the control group. At the 6 month assessment, greater reductions in total health service and time costs were seen in the intervention group; however, cumulative costs over this period were higher (US $627 per patient vs $526 in the control group). Five patients in the intervention group had mild extrapyramidal side effects.
Interpretation: A collaborative shared care delivered by TFH and conventional health-care providers for people with psychosis was effective and cost-effective. The model of care offers the prospect of scaling up improved care to this vulnerable population in settings with low resources.
Funding: US National Institute of Mental Health.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of Interest
We declare no conflicting of interests.
Figures
Comment in
-
A leap of faith for more effective mental health care.Lancet. 2020 Aug 29;396(10251):584-585. doi: 10.1016/S0140-6736(20)31295-2. Lancet. 2020. PMID: 32861294 No abstract available.
References
-
- Whiteford HA, Degenhardt L, Rehm J, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. The Lancet 2013; 382(9904): 1575–86. - PubMed
-
- Gureje O, Nortje G, Makanjuola V, Oladeji BD, Seedat S, Jenkins R. The role of global traditional and complementary systems of medicine in the treatment of mental health disorders. Lancet Psychiatry 2015; 2(2): 168–77. - PubMed
-
- Saeed K, Gater R, Hussain A, Mubbashar M. The prevalence, classification and treatment of mental disorders among attenders of native faith healers in rural Pakistan. Social Psychiatry and Psychiatric Epidemiology 2000; 35: 480–5. - PubMed
-
- van der Watt ASJ, Nortje G, Kola L, et al. Collaboration Between Biomedical and Complementary and Alternative Care Providers: Barriers and Pathways. Qualitative Health Research 2017; 27(14): 2177–88. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
