

NRG Oncology Updated International Consensus Atlas on Pelvic Lymph Node Volumes for Intact and Postoperative Prostate Cancer
- PMID: 32861817
- PMCID: PMC7736505
- DOI: 10.1016/j.ijrobp.2020.08.034
NRG Oncology Updated International Consensus Atlas on Pelvic Lymph Node Volumes for Intact and Postoperative Prostate Cancer
Abstract
Purpose: In 2009, the Radiation Therapy Oncology Group (RTOG) genitourinary members published a consensus atlas for contouring prostate pelvic nodal clinical target volumes (CTVs). Data have emerged further informing nodal recurrence patterns. The objective of this study is to provide an updated prostate pelvic nodal consensus atlas.
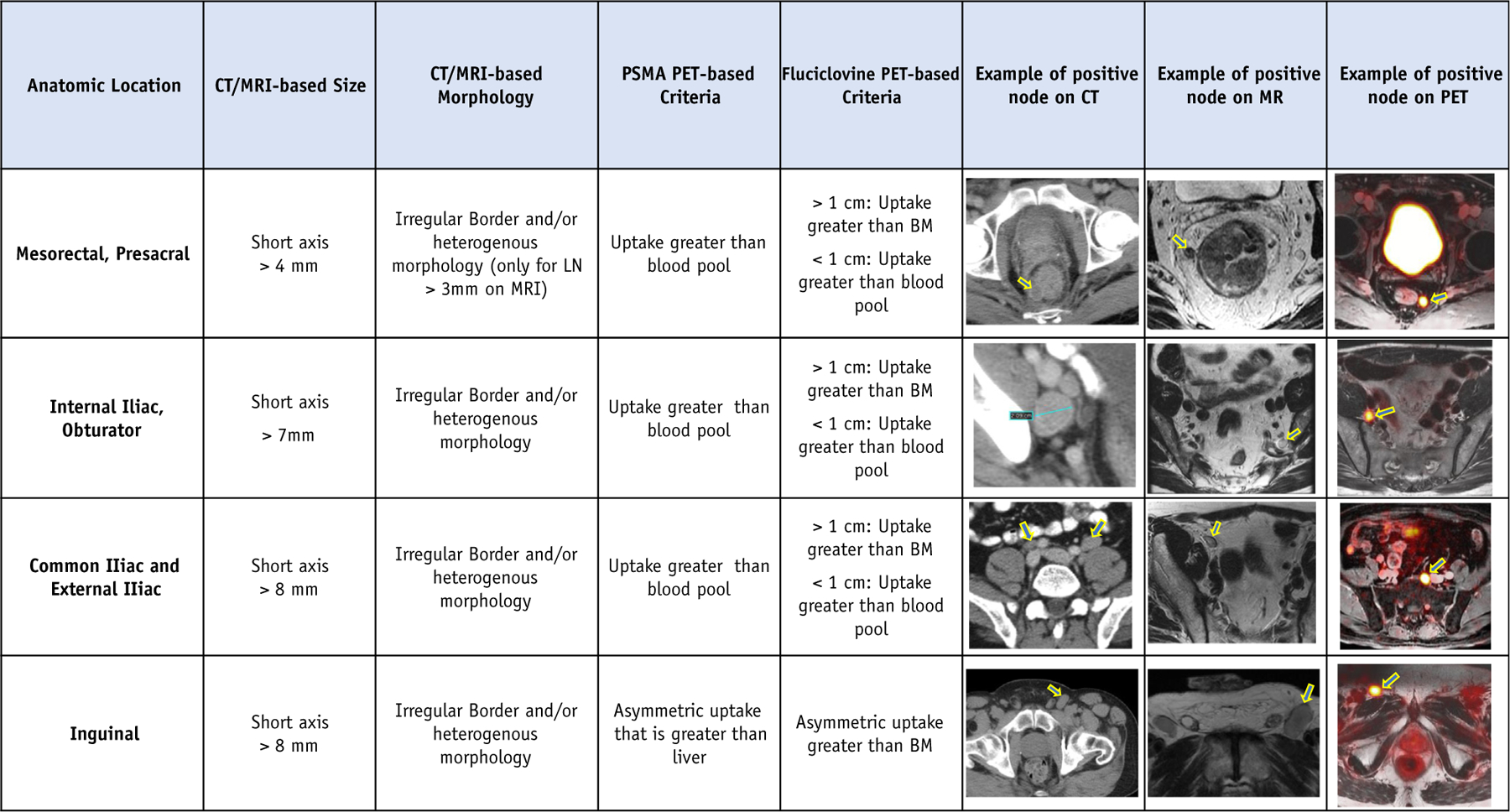
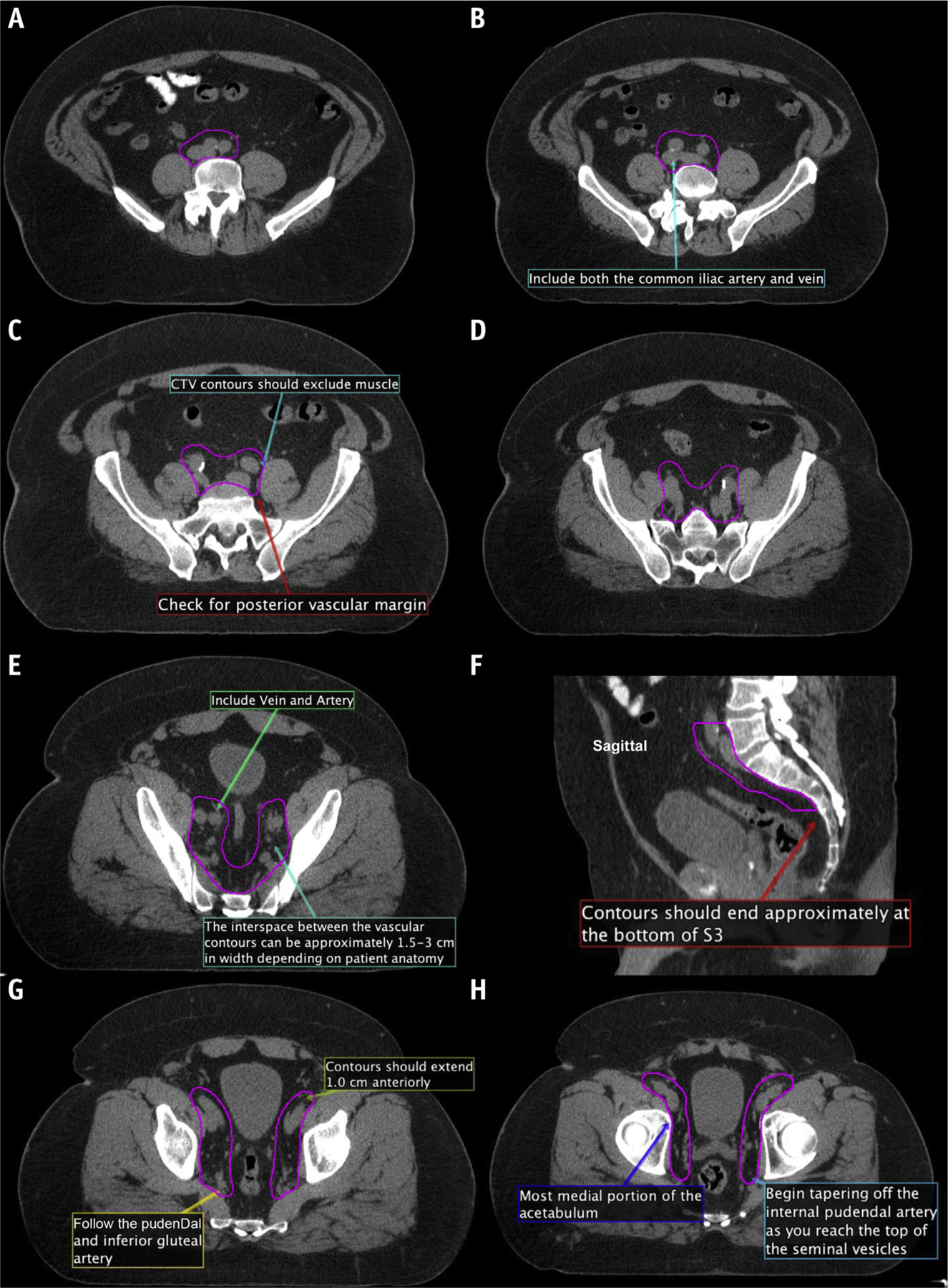
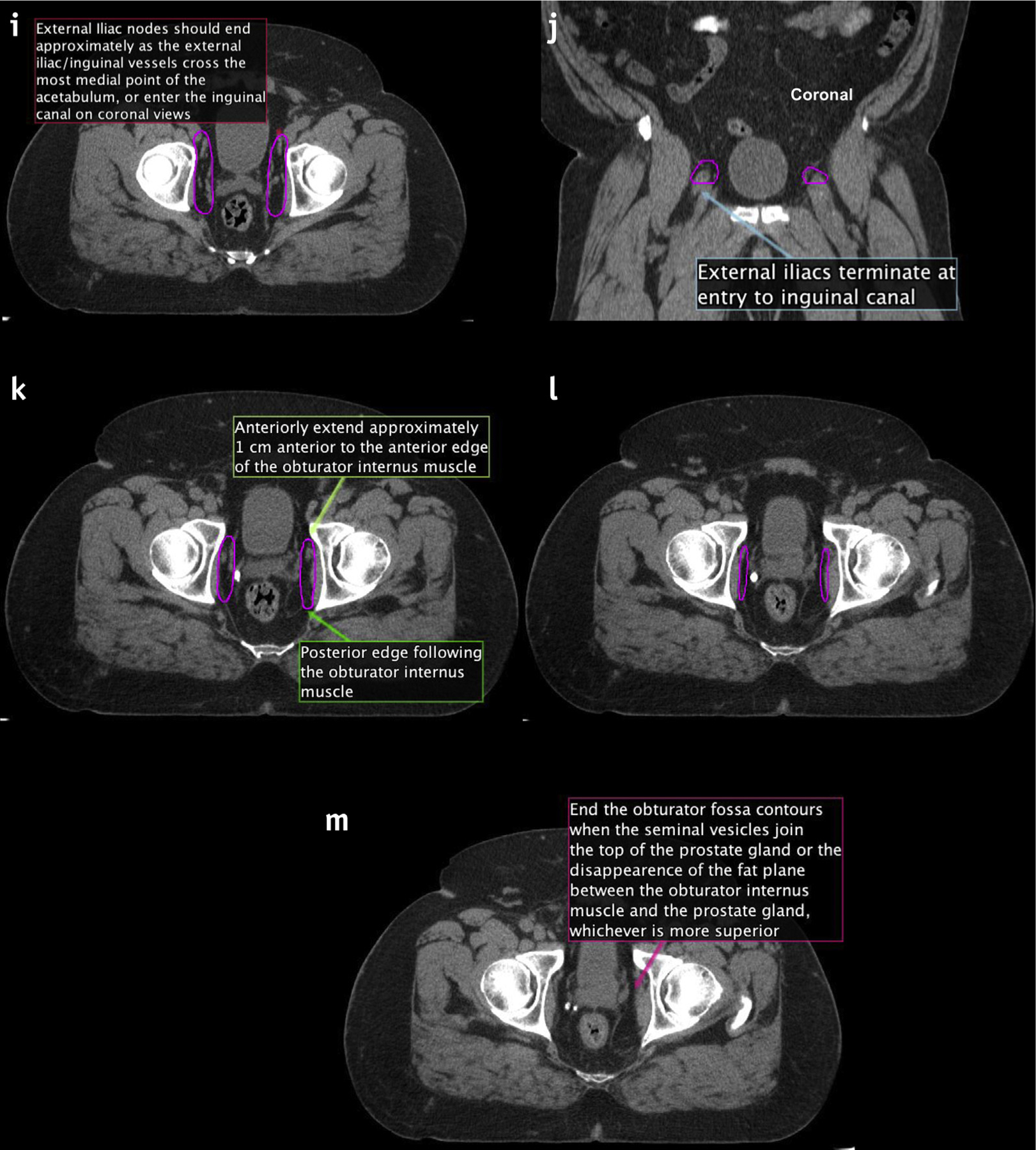
Methods and materials: A literature review was performed abstracting data on nodal recurrence patterns. Data were presented to a panel of international experts, including radiation oncologists, radiologists, and urologists. After data review, participants contoured nodal CTVs on 3 cases: postoperative, intact node positive, and intact node negative. Radiation oncologist contours were analyzed qualitatively using count maps, which provided a visual assessment of controversial regions, and quantitatively analyzed using Sorensen-Dice similarity coefficients and Hausdorff distances compared with the 2009 RTOG atlas. Diagnostic radiologists generated a reference table outlining considerations for determining clinical node positivity.
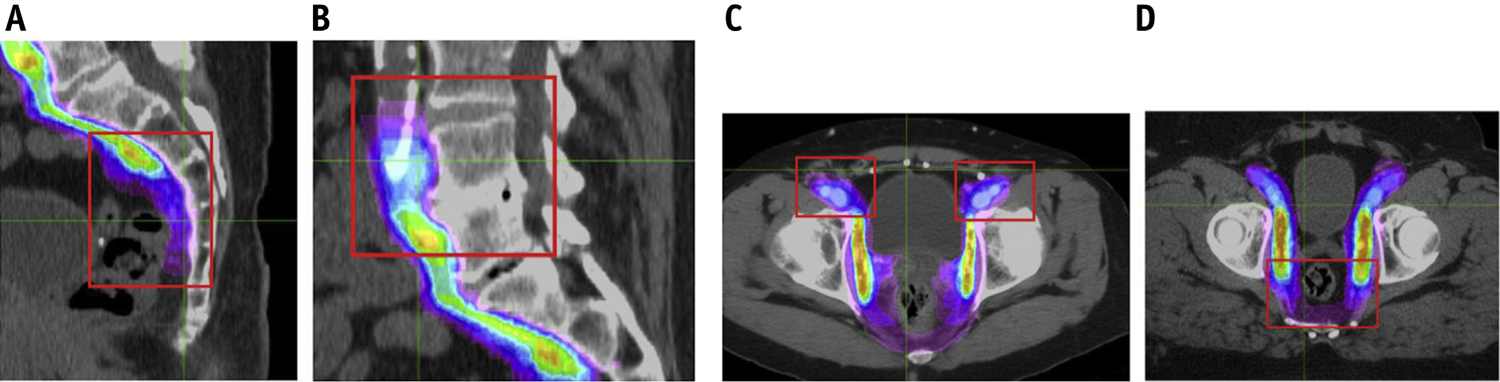
Results: Eighteen radiation oncologists' contours (54 CTVs) were included. Two urologists' volumes were examined in a separate analysis. The mean CTV for the postoperative case was 302 cm3, intact node positive case was 409 cm3, and intact node negative case was 342 cm3. Compared with the original RTOG consensus, the mean Sorensen-Dice similarity coefficient for the postoperative case was 0.63 (standard deviation [SD] 0.13), the intact node positive case was 0.68 (SD 0.13), and the intact node negative case was 0.66 (SD 0.18). The mean Hausdorff distance (in cm) for the postoperative case was 0.24 (SD 0.13), the intact node positive case was 0.23 (SD 0.09), and intact node negative case was 0.33 (SD 0.24). Four regions of CTV controversy were identified, and consensus for each of these areas was reached.
Conclusions: Discordance with the 2009 RTOG consensus atlas was seen in a group of experienced NRG Oncology and international genitourinary radiation oncologists. To address areas of variability and account for new data, an updated NRG Oncology consensus contour atlas was developed.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures
Comment in
-
In regard to Hall et al and Small et al.Int J Radiat Oncol Biol Phys. 2021 Mar 15;109(4):1125-1126. doi: 10.1016/j.ijrobp.2020.11.043. Int J Radiat Oncol Biol Phys. 2021. PMID: 33610294 No abstract available.
-
In Regard to Hall et al.Int J Radiat Oncol Biol Phys. 2021 Jun 1;110(2):619-620. doi: 10.1016/j.ijrobp.2021.01.040. Int J Radiat Oncol Biol Phys. 2021. PMID: 33989588 No abstract available.
-
In Reply to Onal et al.Int J Radiat Oncol Biol Phys. 2021 Jun 1;110(2):620-621. doi: 10.1016/j.ijrobp.2021.01.039. Int J Radiat Oncol Biol Phys. 2021. PMID: 33989589 No abstract available.
References
-
- Pollack A, Karrison T, Balogh JA, Low D, Bruner D. Short term androgen deprivation therapy without or with pelvic lymph node treatment added to prostate bed only salvage radiotherapy: The NRG Oncology/RTOG 0534 SPPORT trial. Int J Radiat Oncol Biol Phys 2018;102:1605.
-
- Lieng H, Kneebone A, Hayden AJ, et al. Radiotherapy for node-positive prostate cancer: 2019 recommendations of the Australian and New Zealand Radiation Oncology Genito-Urinary group. Radiother Oncol 2019;140:68–75. - PubMed
-
- Heidenreich A, Bastian PJ, Bellmunt J, et al. EAU guidelines on prostate cancer. Part 1: screening, diagnosis, and local treatment with curative intent-update 2013. Eur Urol 2014;65:124–137. - PubMed
-
- Mohler JL, Antonarakis ES, Armstrong AJ, et al. Prostate cancer, version 2.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 2019;17:479–505. - PubMed
-
- Roach M 3rd, DeSilvio M, Valicenti R, et al. Whole-pelvis, “minipelvis,” or prostate-only external beam radiotherapy after neoadjuvant and concurrent hormonal therapy in patients treated in the Radiation Therapy Oncology Group 9413 trial. Int J Radiat Oncol Biol Phys 2006;66:647–653. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
