

The impact of coronavirus disease 2019 on the practice of thoracic oncology surgery: a survey of members of the European Society of Thoracic Surgeons (ESTS)
- PMID: 32862224
- PMCID: PMC7499623
- DOI: 10.1093/ejcts/ezaa284
The impact of coronavirus disease 2019 on the practice of thoracic oncology surgery: a survey of members of the European Society of Thoracic Surgeons (ESTS)
Abstract
Objectives: There is widespread acknowledgement that coronavirus disease 2019 (COVID-19) has disrupted surgical services. The European Society of Thoracic Surgeons (ESTS) sent out a survey to assess what impact the COVID-19 pandemic has had on the practice of thoracic oncology surgery.
Methods: All ESTS members were invited (13-20 April 2020) to complete an online questionnaire of 26 questions, designed by the ESTS learning affairs committee.
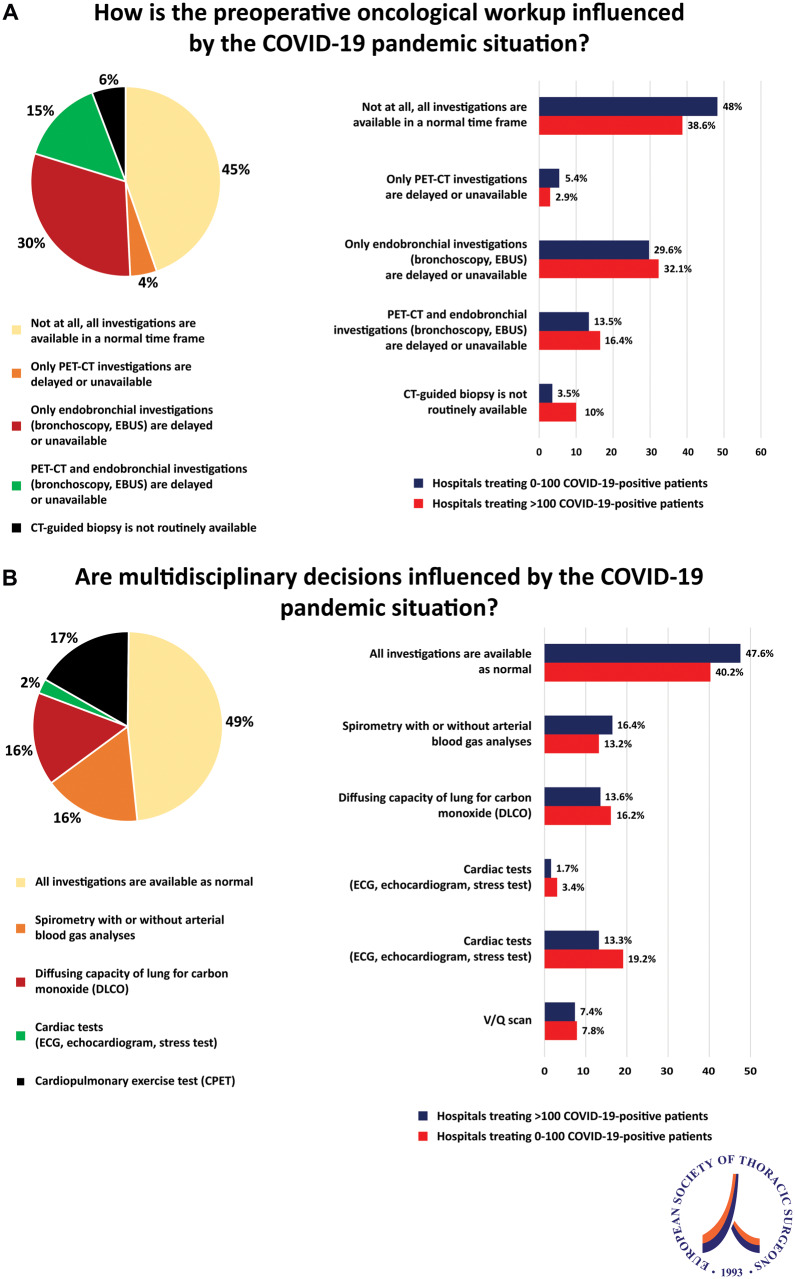
Results: The response rate was 23.0% and the completeness rate was 91.2%. The number of treated COVID-positive cases per hospital varied from fewer than 20 cases (30.6%) to more than 200 cases (22.7%) per hospital. Most hospitals (89.1%) postponed surgical procedures. All hospitals performed patient screening with a nasopharyngeal swab, but only 6.7% routinely tested health care workers. A total of 20% of respondents reported that multidisciplinary meetings were completely cancelled and 66%, that multidisciplinary decisions were not different from normal practice. Trends were recognized in prioritizing surgical patients based on age (younger than 70), type of surgery (lobectomy or less), size of tumour (T1-2) and lymph node involvement (N1). Sixty-three percent of respondents reported that surgeons were involved in daily care of COVID-19-positive patients. Fifty-three percent mentioned that full personal protective equipment was available to them when treating a COVID-19-positive patient.
Conclusions: The COVID-19 pandemic has created issues for the safety of health care workers, and surgeons have been forced to change their routine practice. However, there was no consensus about surgical priorities in lung cancer patients, demonstrating the need for the production of specific guidelines.
Keywords: (MEsH) Survey; Coronavirus disease 2019; Organization and administration; Pandemic; Thoracic surgery.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery. All rights reserved.
Figures






References
-
- Global Covid-19 Case Fatality Rates. CEBM. https://www.cebm.net/global-covid-19-case-fatality-rates/ (24 April 2020, date last accessed).
-
- Einav S, Hick JL, Hanfling D, Erstad BL, Toner ES, Branson RD. et al. Surge capacity logistics: care of the critically ill and injured during pandemics and disasters: CHEST consensus statement. Chest 2014;146:e17S. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
