

Acute pulmonary embolism multimodality imaging prior to endovascular therapy
- PMID: 32862293
- PMCID: PMC7456521
- DOI: 10.1007/s10554-020-01980-9
Acute pulmonary embolism multimodality imaging prior to endovascular therapy
Abstract
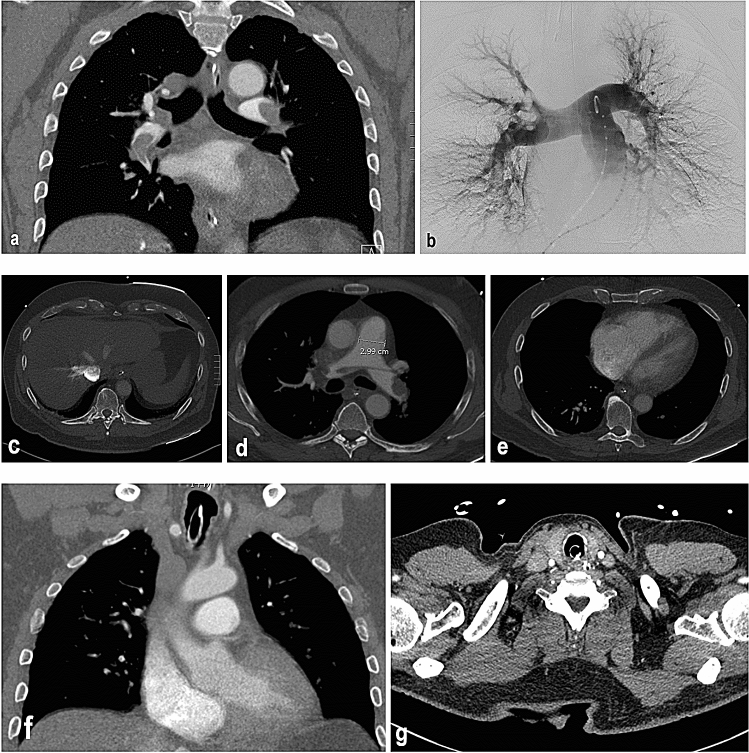
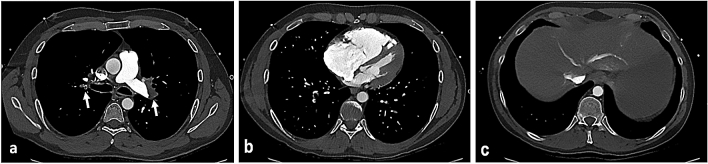
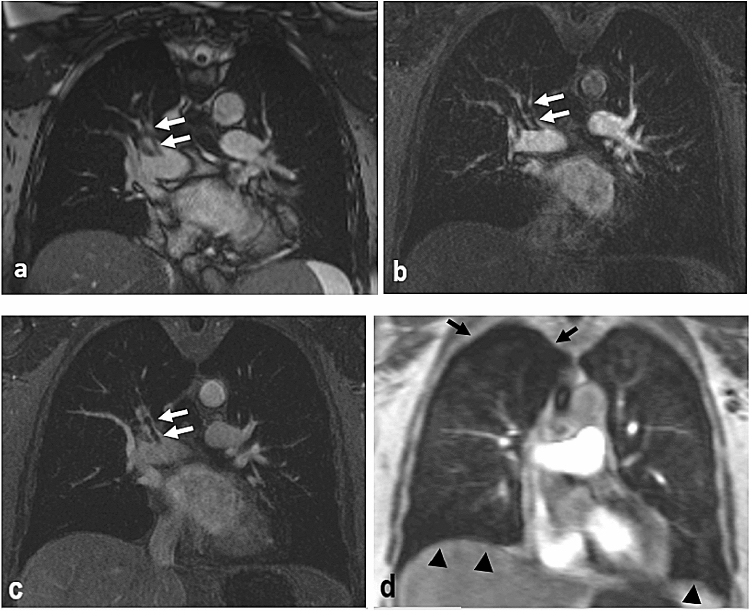
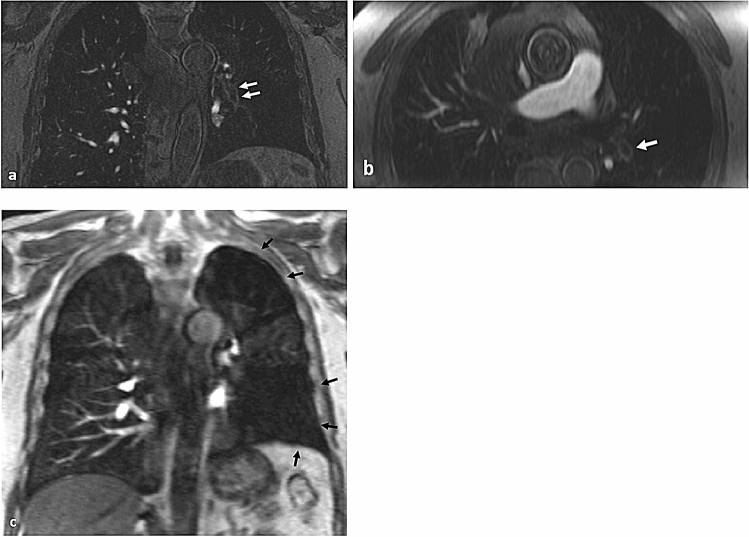
The manuscript discusses the application of CT pulmonary angiography, ventilation-perfusion scan, and magnetic resonance angiography to detect acute pulmonary embolism and to plan endovascular therapy. CT pulmonary angiography offers high accuracy, speed of acquisition, and widespread availability when applied to acute pulmonary embolism detection. This imaging modality also aids the planning of endovascular therapy by visualizing the number and distribution of emboli, determining ideal intra-procedural catheter position for treatment, and signs of right heart strain. Ventilation-perfusion scan and magnetic resonance angiography with and without contrast enhancement can also aid in the detection and pre-procedural planning of endovascular therapy in patients who are not candidates for CT pulmonary angiography.
Keywords: Acute pulmonary embolism; Computed tomography pulmonary angiography; Magnetic resonance angiography; Ventilation–perfusion scan.
Conflict of interest statement
The authors declares that they have no conflict of interest.
Figures



References
-
- Raja AS, Greenberg JO, Qaseem A, Denberg TD, Fitterman N, Schuur JD, for the Clinical Guidelines Committee of the American College of Physicians Evaluation of patients with suspected acute pulmonary embolism: best practice advice from the Clinical Guidelines Committee of the American College of Physicians. Ann Intern Med. 2015;163:701. doi: 10.7326/M14-1772. - DOI - PubMed
-
- Konstantinides SV, Torbicki A, Agnelli G, Danchin N, Fitzmaurice D, Galiè N, Gibbs JSR, Huisman MV, Humbert M, Kucher N, Lang I, Lankeit M, Lekakis J, Maack C, Mayer E, Meneveau N, Perrier A, Pruszczyk P, Rasmussen LH, Schindler TH, Svitil P, Vonk Noordegraaf A, Zamorano JL, Zompatori M, Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC) 2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014;35:3033–3069. doi: 10.1093/eurheartj/ehu283. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
