

Blast polytrauma with hemodynamic shock, hypothermia, hypoventilation and systemic inflammatory response: description of a new porcine model
- PMID: 32862315
- PMCID: PMC7456397
- DOI: 10.1007/s00068-020-01476-0
Blast polytrauma with hemodynamic shock, hypothermia, hypoventilation and systemic inflammatory response: description of a new porcine model
Abstract
Purpose: In the past decade blast injuries have become more prevalent. Blast trauma may cause extensive injuries requiring improved early resuscitation and prevention of haemorrhage. Randomized prospective trials are logistically and ethically challenging, and large animal models are important for further research efforts. Few severe blast trauma models have been described, which is why we aimed to establish a comprehensive polytrauma model in accordance with the criteria of the Berlin definition of polytrauma and with a survival time of > 2 h. Multiple blast injuries to the groin and abdomen were combined with hypoperfusion, respiratory and metabolic acidosis, hypoventilation, hypothermia and inflammatory response. The model was compared to lung contusion and haemorrhage.
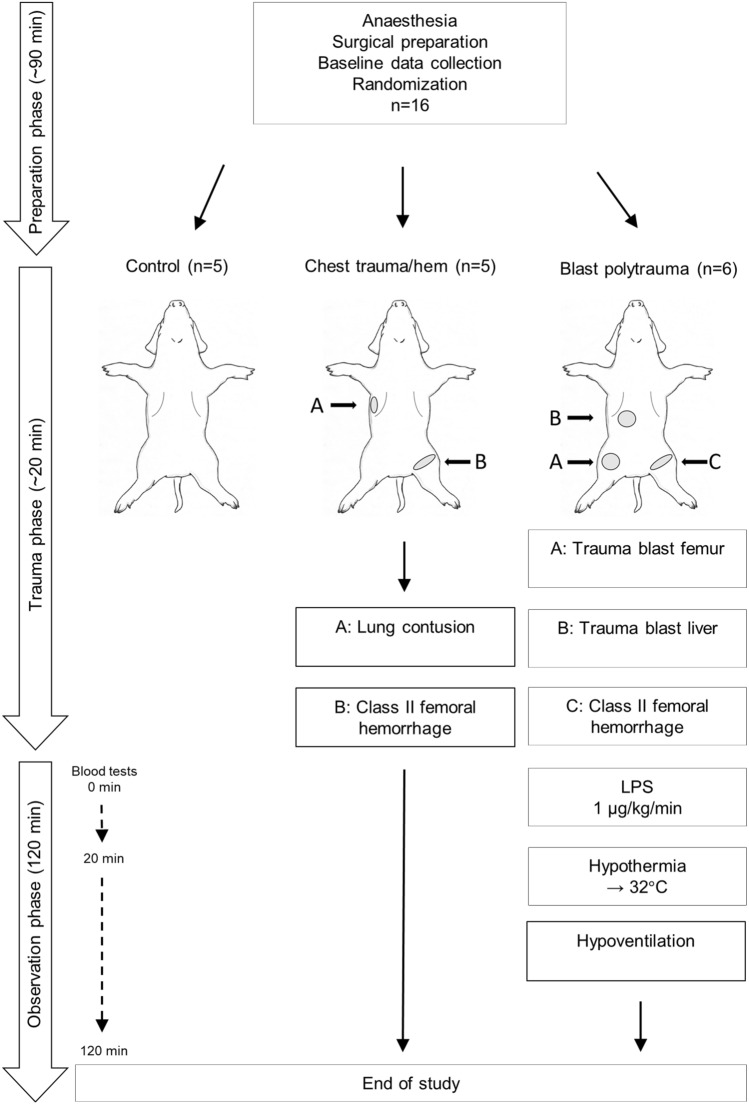
Methods: 16 landrace swine (mean weight 60.5 kg) were randomized to "control" (n = 5), "chest trauma/hem" by lung contusion and class II haemorrhage (n = 5), and "blast polytrauma" caused by multiple blast injuries to the groin and abdomen, class II haemorrhage, lipopolysaccharide (LPS) infusion and hypothermia 32 °C (n = 6).
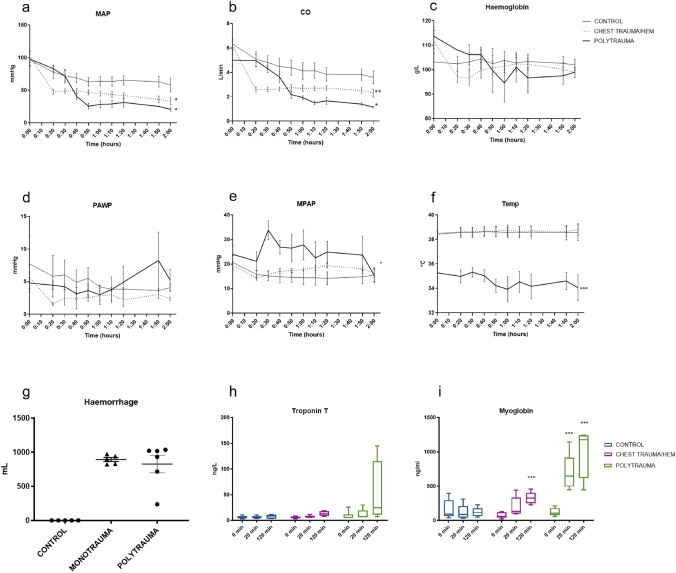
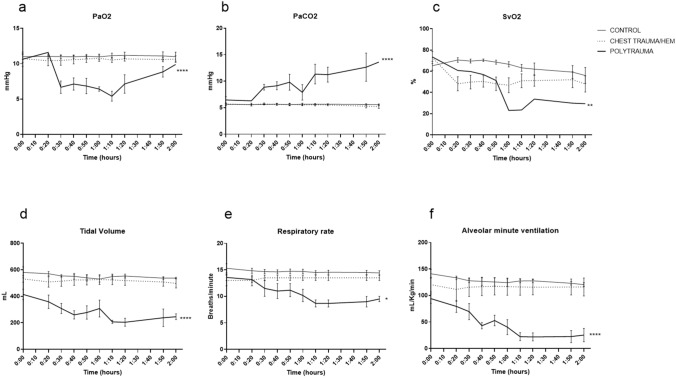
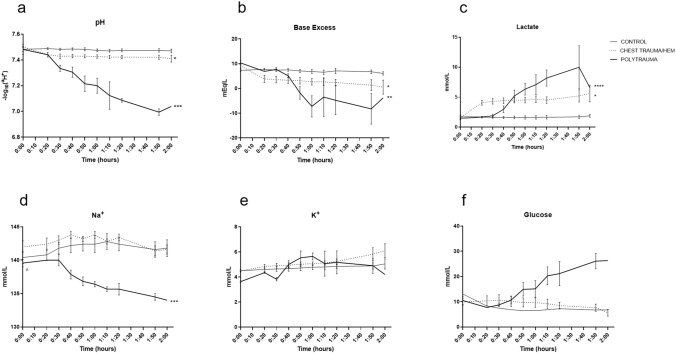
Results: The blast polytrauma group had an Injury Severity Score of 57 which resulted in haemodynamic shock, hypothermia, respiratory and metabolic acidosis and inflammatory response. The chest trauma/hem group had an Injury Severity Score of 9 and less profound physiologic effects. Physiologic parameters presented a dose-response relationship corresponding to the trauma levels.
Conclusion: A comprehensive blast polytrauma model fulfilling the Berlin polytrauma criteria, with a high trauma load and a survival time of > 2 h was established. A severe, but consistent, injury profile was accomplished enabling the addition of experimental interventions in future studies, particularly of immediate resuscitation efforts including whole blood administration, trauma packing and haemostasis.
Keywords: Blast injury; Haemorrhage; Polytrauma; Porcine model.
© 2020. The Author(s).
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- GBD Causes of Death Collaborators Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–1788. doi: 10.1016/s0140-6736(18)32203-7. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
