

Analysis of Mirrored Psychophysiological Change of Cardiac Surgery Team Members During Open Surgery
- PMID: 32863172
- PMCID: PMC7904574
- DOI: 10.1016/j.jsurg.2020.08.012
Analysis of Mirrored Psychophysiological Change of Cardiac Surgery Team Members During Open Surgery
Abstract
Objective: Mirrored psychophysiological change in cognitive workload indices may reflect shared mental models and effective healthcare team dynamics. In this exploratory analysis, we investigated the frequency of mirrored changes, defined as concurrent peaks in heart rate variability (HRV) across team members, during cardiac surgery.
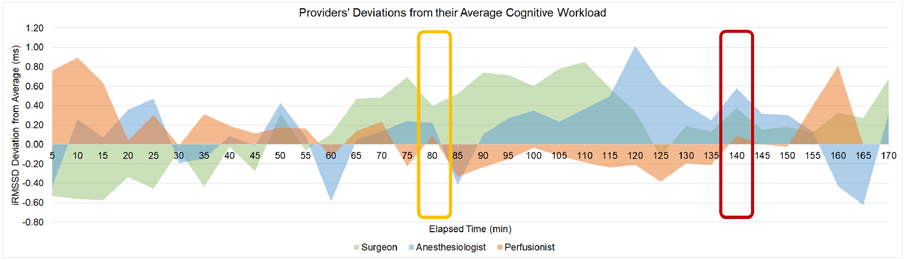
Design: Objective cognitive workload was evaluated via HRV collected from the primary surgical team during cardiac surgery cases (N = 15). Root mean square of the successive differences (RMSSD) was calculated as the primary HRV measure. Procedures were divided into consecutive nonoverlapping 5-minute segments, and RMSSD along with deviations from RMSSD were calculated for each segment. Segments with positive deflections represent above-average cognitive workload. Positive deflections and peaks across dyads within the same segment were counted.
Setting: Data collection for this study took place in the cardiovascular operating room during live surgeries.
Participants: Physiological data were collected and analyzed from the attending surgeon, attending anesthesiologist, and primary perfusionist involved with the recorded cases.
Results: Of the 641 five-minute segments analyzed, 325 (50.7%) were positive deflections above average, concurrently across at least 2 team members. Within the 325 positive deflections, 26 (8%) represented concurrent peaks in HRV across at least 2 active team members. Mirrored peaks across team members were observed most commonly during the coronary anastomoses or valve replacement phase (N = 12).
Conclusions: In this pilot study, mirrored physiological responses representing peaks in cognitive workload were observed uncommonly across dyads of cardiac surgery team members (1.73 peaks/case on average). Almost half of these occurred during the most technically demanding phases of cardiac surgery, which may underpin teamwork quality. Future work should investigate interactions between technical and nontechnical performance surrounding times of mirrored peaks and expand the sample size.
Keywords: cardiac surgery; cognitive workload; heart rate variability; patient safety.
Copyright © 2020 Association of Program Directors in Surgery. All rights reserved.
Conflict of interest statement
Declaration of Interest
None.
Figures
Similar articles
-
The Cognitive Relevance of a Formal Pre-incision Time-out in Surgery.ECCE. 2021 Apr;2021:17. doi: 10.1145/3452853.3452867. Epub 2021 Apr 26. ECCE. 2021. PMID: 34676380 Free PMC article.
-
First Reported Use of Team Cognitive Workload for Root Cause Analysis in Cardiac Surgery.Semin Thorac Cardiovasc Surg. 2019 Autumn;31(3):394-396. doi: 10.1053/j.semtcvs.2018.12.003. Epub 2018 Dec 19. Semin Thorac Cardiovasc Surg. 2019. PMID: 30578828 Free PMC article.
-
Association Between Operating Room Noise and Team Cognitive Workload in Cardiac Surgery.IEEE Conf Cogn Comput Asp Situat Manag. 2022 Jun;2022:89-93. doi: 10.1109/cogsima54611.2022.9830675. Epub 2022 Jul 22. IEEE Conf Cogn Comput Asp Situat Manag. 2022. PMID: 35984653 Free PMC article.
-
[Assessment method of cognitive load and stress inducer factors of surgeons and anesthetists in the operating room].J Fr Ophtalmol. 2023 May;46(5):536-551. doi: 10.1016/j.jfo.2022.11.021. Epub 2023 Apr 16. J Fr Ophtalmol. 2023. PMID: 37068974 Review. French.
-
Can Simulated Team Tasks be Used to Improve Nontechnical Skills in the Operating Room?J Surg Educ. 2016 Nov-Dec;73(6):e42-e47. doi: 10.1016/j.jsurg.2016.06.004. Epub 2016 Aug 1. J Surg Educ. 2016. PMID: 27491863 Review.
Cited by
-
A novel multimodal, intraoperative cognitive workload assessment of cardiac surgery team members.J Thorac Cardiovasc Surg. 2025 Jul;170(1):287-296. doi: 10.1016/j.jtcvs.2024.07.050. Epub 2024 Jul 29. J Thorac Cardiovasc Surg. 2025. PMID: 39084333
-
Episodes of strain experienced in the operating room: impact of the type of surgery, the profession and the phase of the operation.BMC Surg. 2020 Dec 7;20(1):318. doi: 10.1186/s12893-020-00937-y. BMC Surg. 2020. PMID: 33287776 Free PMC article.
-
Sensors for Continuous Monitoring of Surgeon's Cognitive Workload in the Cardiac Operating Room.Sensors (Basel). 2020 Nov 19;20(22):6616. doi: 10.3390/s20226616. Sensors (Basel). 2020. PMID: 33227967 Free PMC article.
-
Surgical Sabermetrics: A Scoping Review of Technology-enhanced Assessment of Nontechnical Skills in the Operating Room.Ann Surg. 2024 Jun 1;279(6):973-984. doi: 10.1097/SLA.0000000000006211. Epub 2024 Jan 23. Ann Surg. 2024. PMID: 38258573 Free PMC article.
-
Cognitive Engineering to Improve Patient Safety and Outcomes in Cardiothoracic Surgery.Semin Thorac Cardiovasc Surg. 2020 Spring;32(1):1-7. doi: 10.1053/j.semtcvs.2019.10.011. Epub 2019 Oct 17. Semin Thorac Cardiovasc Surg. 2020. PMID: 31629782 Free PMC article. Review.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
