

[Inflammation, malnutrition, and SARS-CoV-2 infection: a disastrous combination]
- PMID: 32863403
- PMCID: PMC7566798
- DOI: 10.1016/j.rce.2020.07.007
[Inflammation, malnutrition, and SARS-CoV-2 infection: a disastrous combination]
Abstract
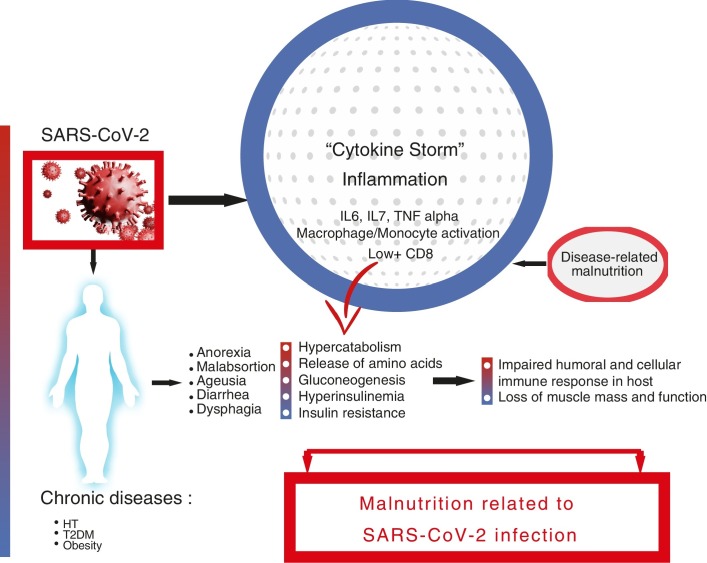
SARS-CoV-2 infection is associated with a high risk of malnutrition, mainly due to increased nutritional requirements and the presence of a severe and universal inflammatory state. Associated symptoms contribute to hyporexia, which perpetuates the negative nutritional balance. Furthermore, dysphagia, especially post-intubation, worsens, and makes intake unsafe. This risk is greater in elderly and multimorbid patients. Inflammation to varying degrees is the common link between COVID-19 and the onset of malnutrition, and it is more correct to refer to disease-related malnutrition (DRM). DRM worsens the poor prognosis of SARS-CoV-2 infection, especially in the most severe cases. Therefore, it is necessary to identify and treat people at risk early, avoiding overexposure and direct contact with the patient. We cannot forget the role that a healthy diet plays in both prevention and recovery after discharge.
Keywords: Citoquine storm; Disease related malnutrition; Inflamation; SARS-CoV-2.
© 2020 Elsevier España, S.L.U. and Sociedad Española de Medicina Interna (SEMI). All rights reserved.
Figures
Similar articles
-
[Inflammation, malnutrition, and SARS-CoV-2 infection: a disastrous combination].Rev Clin Esp. 2020 Nov;220(8):511-517. doi: 10.1016/j.rce.2020.07.007. Epub 2020 Aug 24. Rev Clin Esp. 2020. PMID: 38620641 Free PMC article. Spanish.
-
Approaches to Nutritional Screening in Patients with Coronavirus Disease 2019 (COVID-19).Int J Environ Res Public Health. 2021 Mar 9;18(5):2772. doi: 10.3390/ijerph18052772. Int J Environ Res Public Health. 2021. PMID: 33803339 Free PMC article. Review.
-
Impact of severe SARS-CoV-2 infection on nutritional status and subjective functional loss in a prospective cohort of COVID-19 survivors.BMJ Open. 2021 Jul 14;11(7):e048948. doi: 10.1136/bmjopen-2021-048948. BMJ Open. 2021. PMID: 34261689 Free PMC article.
-
Prevalence of nutritional risk and malnutrition during and after hospitalization for COVID-19 infection: Preliminary results of a single-centre experience.Clin Nutr ESPEN. 2021 Oct;45:351-355. doi: 10.1016/j.clnesp.2021.07.020. Epub 2021 Aug 2. Clin Nutr ESPEN. 2021. PMID: 34620339 Free PMC article.
-
Coronavirus Disease 2019 (COVID-19) and Nutritional Status: The Missing Link?Adv Nutr. 2021 Jun 1;12(3):682-692. doi: 10.1093/advances/nmaa125. Adv Nutr. 2021. PMID: 32975565 Free PMC article. Review.
Cited by
-
A retrospective cohort study on the association between nutritional status and prognosis in COVID-19 patients with severe and critical infection.J Int Med Res. 2024 Nov;52(11):3000605241292326. doi: 10.1177/03000605241292326. J Int Med Res. 2024. PMID: 39506245 Free PMC article.
References
-
- World Health Organization. Rolling update on coronavirus disease (COVID-19): WHO characterizes COVID-19 as a pandemic. 11 March 2020. Available from https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-a....
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
