

Evening and overnight closed-loop control versus 24/7 continuous closed-loop control for type 1 diabetes: a randomised crossover trial
- PMID: 32864597
- PMCID: PMC7453908
- DOI: 10.1016/S2589-7500(19)30218-3
Evening and overnight closed-loop control versus 24/7 continuous closed-loop control for type 1 diabetes: a randomised crossover trial
Abstract
Background: Automated closed-loop control (CLC), known as the "artificial pancreas" is emerging as a treatment option for Type 1 Diabetes (T1D), generally superior to sensor-augmented insulin pump (SAP) treatment. It is postulated that evening-night (E-N) CLC may account for most of the benefits of 24-7 CLC; however, a direct comparison has not been done.
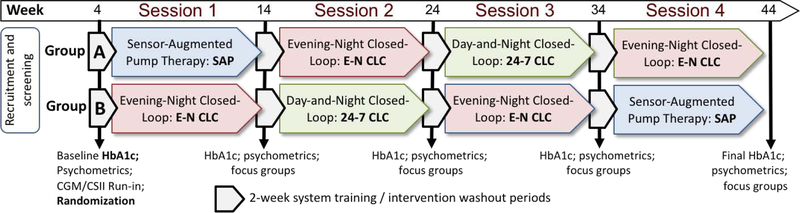
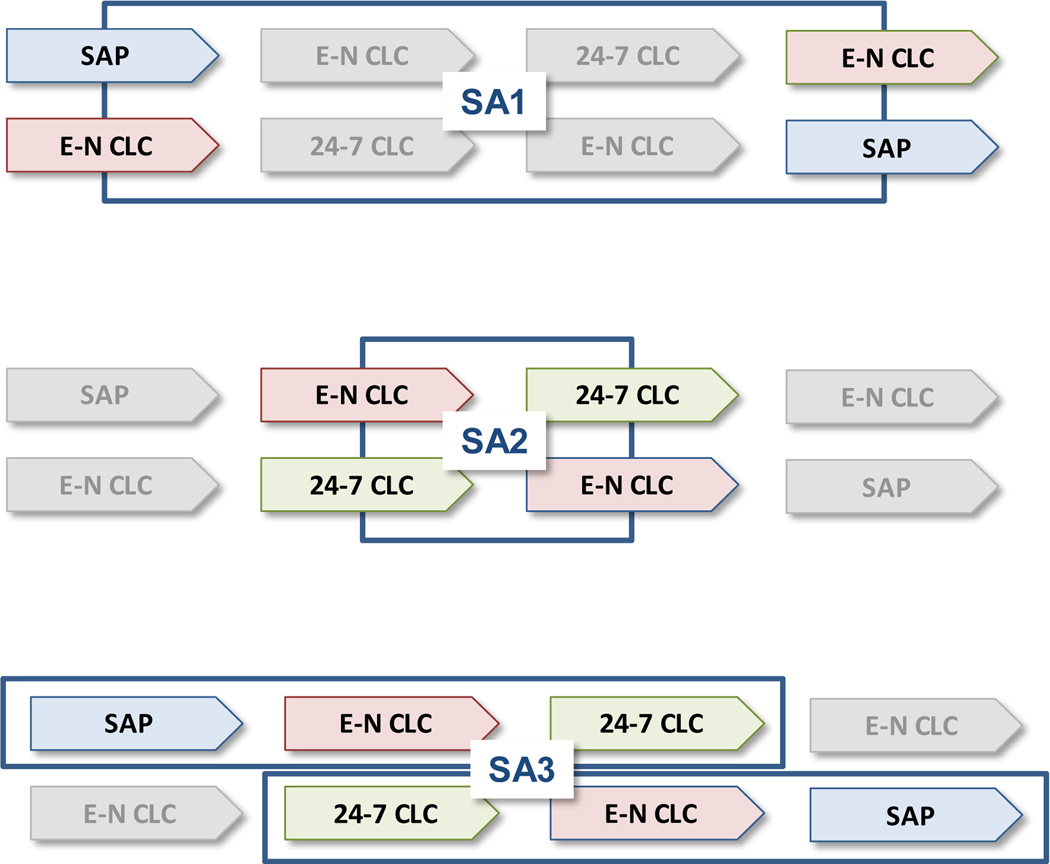
Methods: In this trial (NCT02679287), adults with T1D were randomised 1:1 to two groups, which followed different sequences of four 8-week sessions, resulting in two crossover designs comparing SAP vs E-N CLC and E-N CLC vs 24-7 CLC, respectively. Eligibility: T1D for at least 1 year, using an insulin pump for at least six months, ages 18 years or older. Primary hypothesis: E-N CLC compared to SAP will decrease percent time <70mg/dL (3.9mmol/L) measured by continuous glucose monitoring (CGM) without deterioration in HbA1c. Secondary Hypotheses: 24-7 CLC compared to SAP will increase CGM-measured time in target range (TIR, 70-180mg/dL; 3.9-10mmol/L) and will reduce glucose variability during the day.
Findings: Ninety-three participants were randomised and 80 were included in the analysis, ages 18-69 years; HbA1c levels 5.4-10.6%; 66% female. Compared to SAP, E-N CLC reduced overall time <70mg/dL from 4.0% to 2.2% () resulting in an absolute difference of 1.8% (95%CI: 1.2-2.4%), p<0.0001. This was accompanied by overall reduction in HbA1c from 7.4% at baseline to 7.1% at the end of study, resulting in an absolute difference of 0.3% (95% CI: 0.1-0.4%), p<0.0001. There were 5 severe hypoglycaemia adverse events attributed to user-directed boluses without malfunction of the investigational device, and no diabetic ketoacidosis events.
Interpretation: In type 1 diabetes, evening-night closed-loop control was superior to sensor-augmented pump therapy, achieving most of the glycaemic benefits of 24-7 closed-loop.
Keywords: Artificial Pancreas; Closed-Loop Control (CLC); Continuous Glucose Monitoring (CGM); Continuous Subcutaneous Insulin Infusion (CSII).
Figures
Comment in
-
Closed-loop insulin delivery: understanding when and how it is effective.Lancet Digit Health. 2020 Feb;2(2):e50-e51. doi: 10.1016/S2589-7500(19)30219-5. Epub 2020 Jan 3. Lancet Digit Health. 2020. PMID: 33334557 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous