

Preoperative Risk Assessment: A Poor Predictor of Outcome in Critically ill Elderly with Sepsis After Abdominal Surgery
- PMID: 32864720
- PMCID: PMC7599195
- DOI: 10.1007/s00268-020-05742-5
Preoperative Risk Assessment: A Poor Predictor of Outcome in Critically ill Elderly with Sepsis After Abdominal Surgery
Abstract
Background: Postoperative outcome prediction in elderly is based on preoperative physical status but its predictive value is uncertain. The goal was to evaluate the value of risk assessment performed perioperatively in predicting outcome in case of admission to an intensive care unit (ICU).
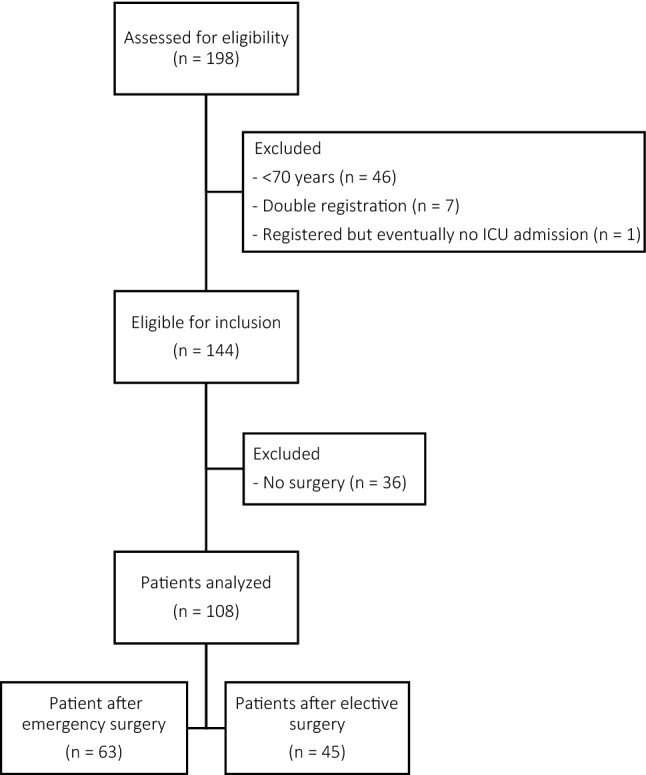
Methods: A total of 108 postsurgical patients were retrospectively selected from a prospectively recorded database of 144 elderly septic patients (>70 years) admitted to the ICU department after elective or emergency abdominal surgery between 2012 and 2017. Perioperative risk assessment scores including Portsmouth Physiological and Operative Severity Score for the enumeration of Mortality (P-POSSUM) and American Society of Anaesthesiologists Physical Status classification (ASA) were determined. Acute Physiology and Chronic Health Evaluation IV (APACHE IV) was obtained at ICU admission.
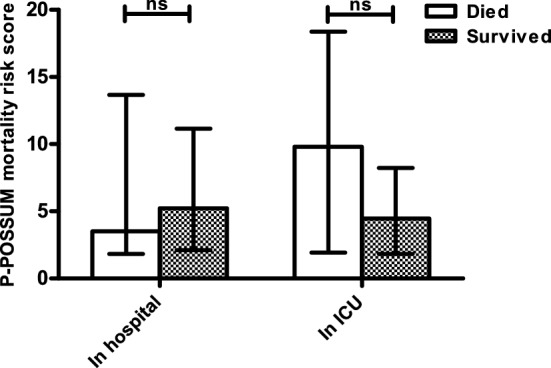
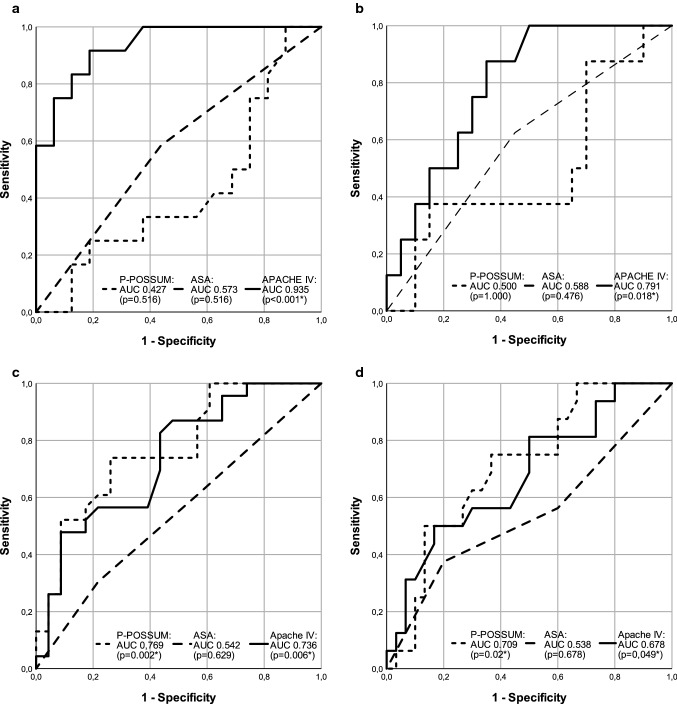
Results: In-hospital mortality was 48.9% in elderly requiring ICU admission after elective surgery (n = 45), compared to 49.2% after emergency surgery (n = 63). APACHE IV significantly predicted in-hospital mortality after complicated elective surgery [area under the curve 0.935 (p < 0.001)] where outpatient ASA physical status and P-POSSUM did not. In contrast, P-POSSUM and APACHE IV significantly predicted in-hospital mortality when based on current physical state in elderly requiring emergency surgery (AUC 0.769 (p = 0.002) and 0.736 (p = 0.006), respectively).
Conclusions: Perioperative risk assessment reflecting premorbid physical status of elderly loses its value when complications occur requiring unplanned ICU admission. Risks in elderly should be re-assessed based on current clinical condition prior to ICU admission, because outcome prediction is more reliable then.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- United Nations DoEaSA, Population Division (2017) World population ageing 2017—highlights 2017, New York
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
