

Predicting Early Warning Signs of Psychotic Relapse From Passive Sensing Data: An Approach Using Encoder-Decoder Neural Networks
- PMID: 32865506
- PMCID: PMC7490673
- DOI: 10.2196/19962
Predicting Early Warning Signs of Psychotic Relapse From Passive Sensing Data: An Approach Using Encoder-Decoder Neural Networks
Abstract
Background: Schizophrenia spectrum disorders (SSDs) are chronic conditions, but the severity of symptomatic experiences and functional impairments vacillate over the course of illness. Developing unobtrusive remote monitoring systems to detect early warning signs of impending symptomatic relapses would allow clinicians to intervene before the patient's condition worsens.
Objective: In this study, we aim to create the first models, exclusively using passive sensing data from a smartphone, to predict behavioral anomalies that could indicate early warning signs of a psychotic relapse.
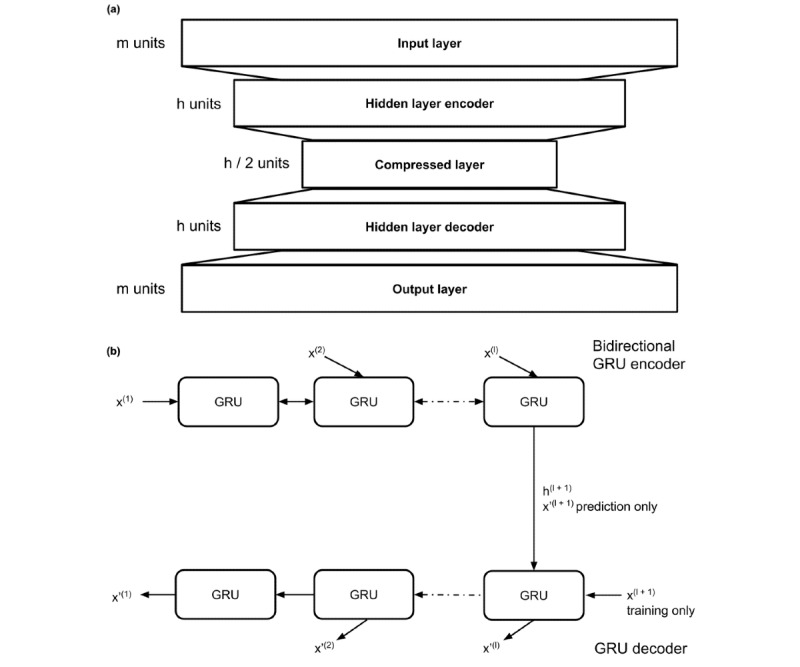
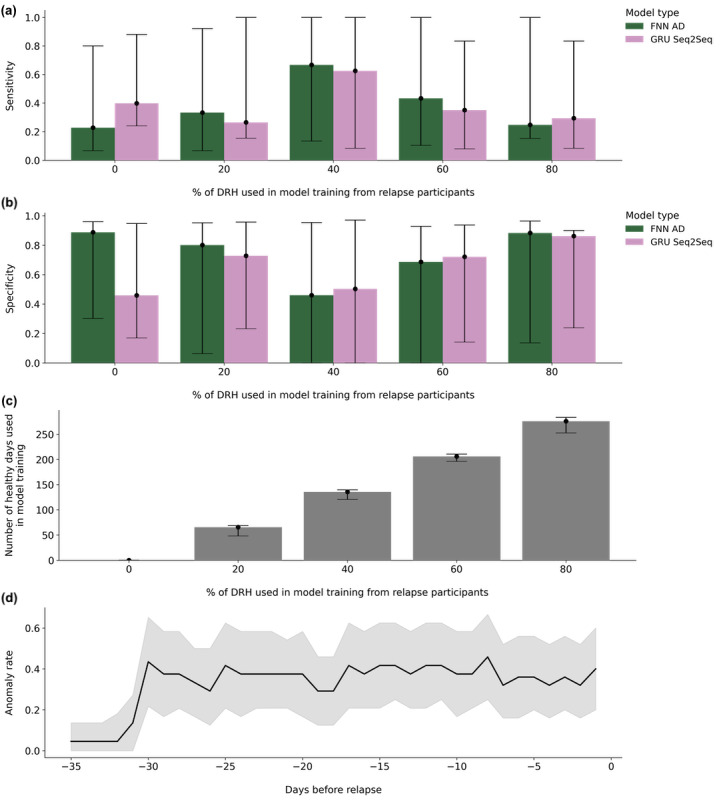
Methods: Data used to train and test the models were collected during the CrossCheck study. Hourly features derived from smartphone passive sensing data were extracted from 60 patients with SSDs (42 nonrelapse and 18 relapse >1 time throughout the study) and used to train models and test performance. We trained 2 types of encoder-decoder neural network models and a clustering-based local outlier factor model to predict behavioral anomalies that occurred within the 30-day period before a participant's date of relapse (the near relapse period). Models were trained to recreate participant behavior on days of relative health (DRH, outside of the near relapse period), following which a threshold to the recreation error was applied to predict anomalies. The neural network model architecture and the percentage of relapse participant data used to train all models were varied.
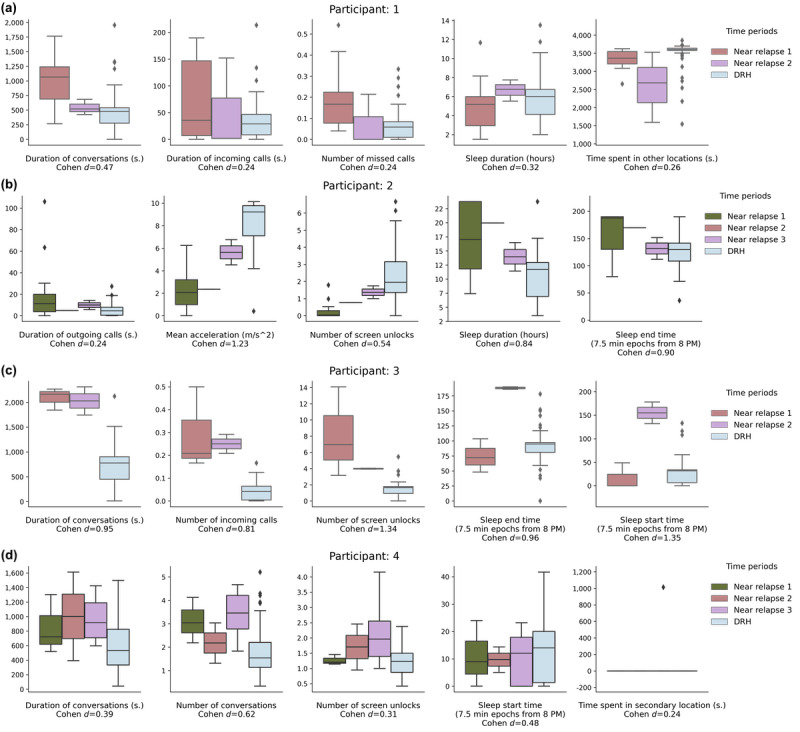
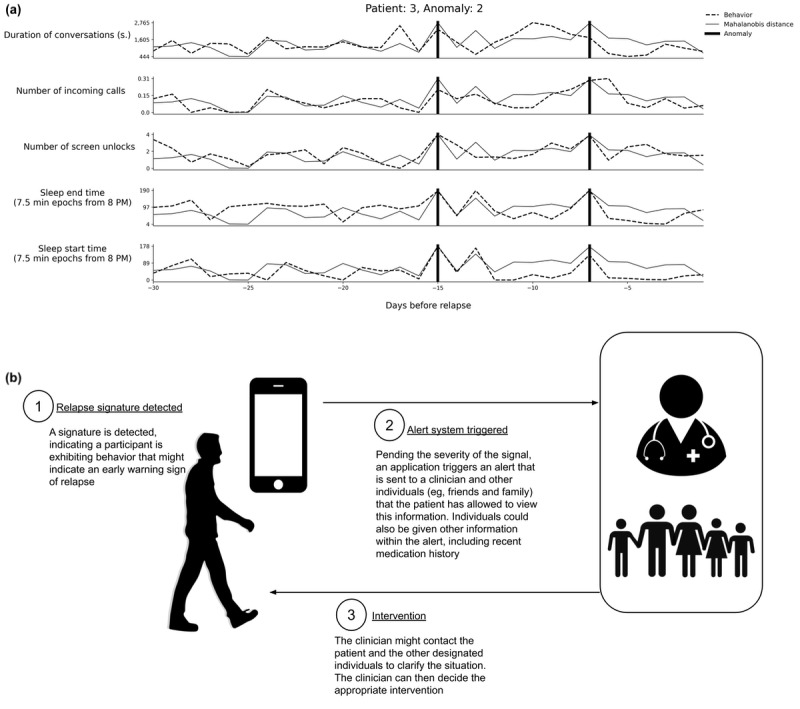
Results: A total of 20,137 days of collected data were analyzed, with 726 days of data (0.037%) within any 30-day near relapse period. The best performing model used a fully connected neural network autoencoder architecture and achieved a median sensitivity of 0.25 (IQR 0.15-1.00) and specificity of 0.88 (IQR 0.14-0.96; a median 108% increase in behavioral anomalies near relapse). We conducted a post hoc analysis using the best performing model to identify behavioral features that had a medium-to-large effect (Cohen d>0.5) in distinguishing anomalies near relapse from DRH among 4 participants who relapsed multiple times throughout the study. Qualitative validation using clinical notes collected during the original CrossCheck study showed that the identified features from our analysis were presented to clinicians during relapse events.
Conclusions: Our proposed method predicted a higher rate of anomalies in patients with SSDs within the 30-day near relapse period and can be used to uncover individual-level behaviors that change before relapse. This approach will enable technologists and clinicians to build unobtrusive digital mental health tools that can predict incipient relapse in SSDs.
Keywords: artificial intelligence; deep learning; digital biomarkers; digital phenotyping; mHealth; machine learning; mental health; mobile health; mobile phone; passive sensing; psychotic disorders; schizophrenia; smartphone applications.
©Daniel A Adler, Dror Ben-Zeev, Vincent W-S Tseng, John M Kane, Rachel Brian, Andrew T Campbell, Marta Hauser, Emily A Scherer, Tanzeem Choudhury. Originally published in JMIR mHealth and uHealth (http://mhealth.jmir.org), 31.08.2020.
Conflict of interest statement
Conflicts of Interest: DBZ has an intervention content licensing agreement with Pear Therapeutics and has a financial interest in FOCUS technology. DBZ has consulted for eQuility, Trusst Health, and Otsuka Pharmaceutical Ltd. JK has received honoraria for lectures and/or consulting from Alkermes, Dainippon, Sumitomo, Sunovion, Janssen, Intracellular Therapies, Lundbeck, Otsuka, Roche, Teva, Neurocrine, LB Pharma, and Merck. JK is a shareholder of Vanguard Research Group and LB Pharma. TC is a co-founder and equity holder of HealthRhythms, Inc. The other authors declare no competing interests.
Figures
References
-
- Emsley R, Chiliza B, Asmal L, Harvey BH. The nature of relapse in schizophrenia. BMC Psychiatry. 2013 Feb 8;13:50. doi: 10.1186/1471-244X-13-50. https://bmcpsychiatry.biomedcentral.com/articles/10.1186/1471-244X-13-50 - DOI - DOI - PMC - PubMed
-
- Eisner E, Drake R, Lobban F, Bucci S, Emsley R, Barrowclough C. Comparing early signs and basic symptoms as methods for predicting psychotic relapse in clinical practice. Schizophr Res. 2018 Feb;192:124–30. doi: 10.1016/j.schres.2017.04.050. https://linkinghub.elsevier.com/retrieve/pii/S0920-9964(17)30259-1 - DOI - PMC - PubMed
-
- Overall JE, Gorham DR. The brief psychiatric rating scale. Psychol Rep. 1962 Jun 1;10(3):799–812. doi: 10.2466/pr0.1962.10.3.799. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
